Xinjian Li, Lin Mi, Juntao Duan, Liyuan Tao, Xinye Xu, Guisong Wang
{"title":"基于默里定律的定量血流比率用于评估 ST 段抬高型心肌梗死患者的非病灶。","authors":"Xinjian Li, Lin Mi, Juntao Duan, Liyuan Tao, Xinye Xu, Guisong Wang","doi":"10.5603/cj.93499","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Revascularization of nonculprit arteries in patients with ST-Segment Elevation Myocardial Infarction (STEMI) is now recommended based on several trials. However, the optimal therapeutic strategy of nonculprit lesions remains unknown. Murray law-based Quantitative Flow Ratio (μQFR) is a novel, non-invasive, vasodilator-free method for evaluating the functional severity of coronary artery stenosis, which has potential applications for nonculprit lesion assessment in STEMI patients.</p><p><strong>Material and methods: </strong>Patients with STEMI who received staged PCI before hospital discharge were enrolled retrospectively. μQFR analyses of nonculprit vessels were performed based on both acute and staged angiography.</p><p><strong>Results: </strong>Eighty-four patients with 110 nonculprit arteries were included. The mean acute μQFR was 0.76 ± 0.18, and the mean staged μQFR was 0.75 ± 0.19. The average period between acute and staged evaluation was 8 days. There was a good correlation (r = 0.719, P < 0.001) between acute μQFR and staged μQFR. The classification agreement was 89.09%. The area under the receiver operator characteristic (ROC) curve for detecting staged μQFR ≤ 0.80 was 0.931.</p><p><strong>Conclusions: </strong>It is feasible to calculate the μQFR during the acute phase of STEMI patients. Acute μQFR and staged μQFR have a good correlation and agreement. The μQFR could be a valuable method for assessing functional significance of nonculprit arteries in STEMI patients.</p>","PeriodicalId":93923,"journal":{"name":"Cardiology journal","volume":" ","pages":"522-527"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11374328/pdf/","citationCount":"0","resultStr":"{\"title\":\"Murray law-based quantitative flow ratio for assessment of nonculprit lesions in patients with ST-segment elevation myocardial infarction.\",\"authors\":\"Xinjian Li, Lin Mi, Juntao Duan, Liyuan Tao, Xinye Xu, Guisong Wang\",\"doi\":\"10.5603/cj.93499\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Revascularization of nonculprit arteries in patients with ST-Segment Elevation Myocardial Infarction (STEMI) is now recommended based on several trials. However, the optimal therapeutic strategy of nonculprit lesions remains unknown. Murray law-based Quantitative Flow Ratio (μQFR) is a novel, non-invasive, vasodilator-free method for evaluating the functional severity of coronary artery stenosis, which has potential applications for nonculprit lesion assessment in STEMI patients.</p><p><strong>Material and methods: </strong>Patients with STEMI who received staged PCI before hospital discharge were enrolled retrospectively. μQFR analyses of nonculprit vessels were performed based on both acute and staged angiography.</p><p><strong>Results: </strong>Eighty-four patients with 110 nonculprit arteries were included. The mean acute μQFR was 0.76 ± 0.18, and the mean staged μQFR was 0.75 ± 0.19. The average period between acute and staged evaluation was 8 days. There was a good correlation (r = 0.719, P < 0.001) between acute μQFR and staged μQFR. The classification agreement was 89.09%. The area under the receiver operator characteristic (ROC) curve for detecting staged μQFR ≤ 0.80 was 0.931.</p><p><strong>Conclusions: </strong>It is feasible to calculate the μQFR during the acute phase of STEMI patients. Acute μQFR and staged μQFR have a good correlation and agreement. The μQFR could be a valuable method for assessing functional significance of nonculprit arteries in STEMI patients.</p>\",\"PeriodicalId\":93923,\"journal\":{\"name\":\"Cardiology journal\",\"volume\":\" \",\"pages\":\"522-527\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11374328/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5603/cj.93499\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5603/cj.93499","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/8 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Murray law-based quantitative flow ratio for assessment of nonculprit lesions in patients with ST-segment elevation myocardial infarction.
Introduction: Revascularization of nonculprit arteries in patients with ST-Segment Elevation Myocardial Infarction (STEMI) is now recommended based on several trials. However, the optimal therapeutic strategy of nonculprit lesions remains unknown. Murray law-based Quantitative Flow Ratio (μQFR) is a novel, non-invasive, vasodilator-free method for evaluating the functional severity of coronary artery stenosis, which has potential applications for nonculprit lesion assessment in STEMI patients.
Material and methods: Patients with STEMI who received staged PCI before hospital discharge were enrolled retrospectively. μQFR analyses of nonculprit vessels were performed based on both acute and staged angiography.
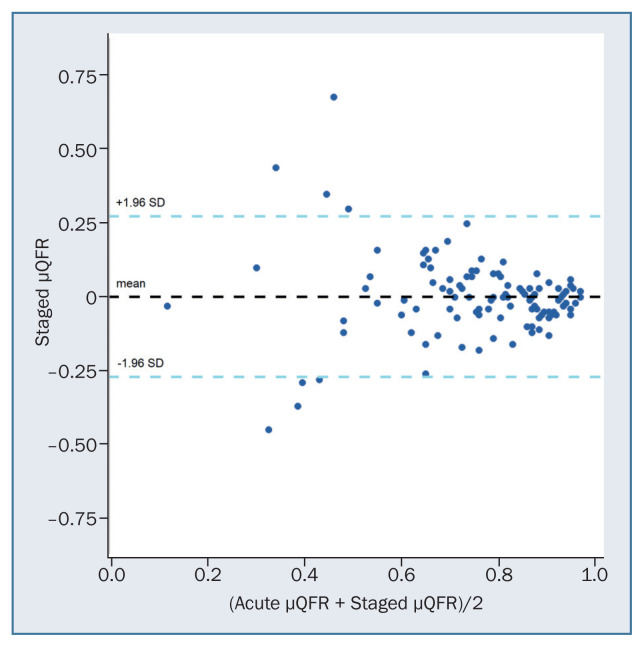
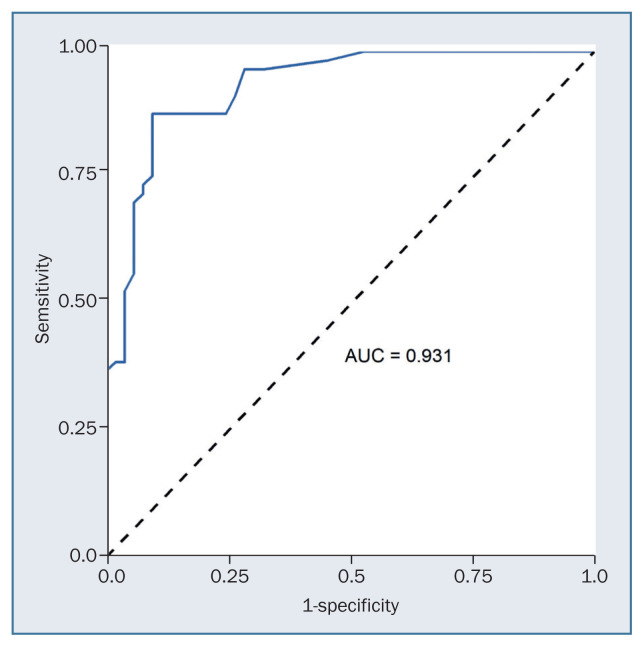
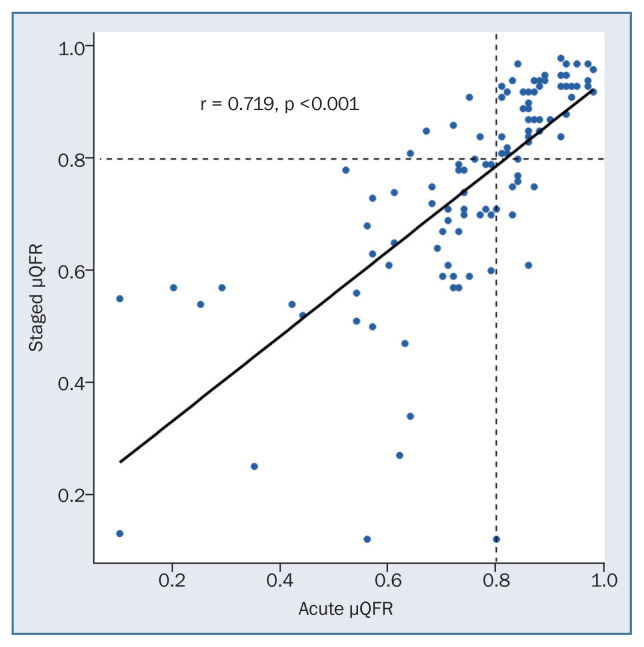
Results: Eighty-four patients with 110 nonculprit arteries were included. The mean acute μQFR was 0.76 ± 0.18, and the mean staged μQFR was 0.75 ± 0.19. The average period between acute and staged evaluation was 8 days. There was a good correlation (r = 0.719, P < 0.001) between acute μQFR and staged μQFR. The classification agreement was 89.09%. The area under the receiver operator characteristic (ROC) curve for detecting staged μQFR ≤ 0.80 was 0.931.
Conclusions: It is feasible to calculate the μQFR during the acute phase of STEMI patients. Acute μQFR and staged μQFR have a good correlation and agreement. The μQFR could be a valuable method for assessing functional significance of nonculprit arteries in STEMI patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


