Dominic Cooper, Rajneesh Kaur, Femi E Ayeni, Guy D Eslick, Senarath Edirimanne
{"title":"甲状腺半切除术后甲状腺功能减退:系统回顾和荟萃分析。","authors":"Dominic Cooper, Rajneesh Kaur, Femi E Ayeni, Guy D Eslick, Senarath Edirimanne","doi":"10.1186/s13044-024-00200-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The incidence of hypothyroidism following hemithyroidectomy and risk factors associated with its occurrence are not completely understood. This systematic review investigated the incidence and risk factors for hypothyroidism, thyroxine supplementation following hemithyroidectomy as well as the course of post-operative hypothyroidism, including the time to hypothyroidism and incidence of transient hypothyroidism.</p><p><strong>Methods: </strong>Searches were conducted in MEDLINE, EMBASE, Scopus, and Cochrane library for studies reporting the incidence of hypothyroidism or thyroxine supplementation following hemithyroidectomy.</p><p><strong>Results: </strong>Sixty-six studies were eligible for inclusion: 36 reported risk factors, and 27 reported post-operative course of hypothyroidism. Median follow-up was 25.2 months. The pooled incidence of hypothyroidism was 29% (95% CI, 25-34%; P<0.001). Transient hypothyroidism occurred in 34% of patients (95% CI, 21-47%; P<0.001). The pooled incidence of thyroxine supplementation was 23% (95% CI, 19-27%; P<0.001), overt hypothyroidism 4% (95% CI, 2-6%, P<0.001). Risk factors for development of hypothyroidism included pre-operative thyroid stimulating hormone (TSH) (WMD, 0.87; 95% CI, 0.75-0.98; P<0.001), TSH ≥ 2 mIU/L (RR, 2.87; 95% CI, 2.43-3.40; P<0.001), female sex (RR, 1.19; 95% CI, 1.08-1.32; P=0.007), age (WMD, 2.29; 95% CI, 1.20-3.38; P<0.001), right sided hemithyroidectomy (RR, 1.35; 95% CI, 1.10-1.65, P=0.003), the presence of autoantibodies anti-TPO (RR, 1.92; 95% CI, 1.49-2.48; P<0.001), anti-Tg (RR, 1.53; 95% CI, 1.40-1.88; P<0.001), and Hashimoto's thyroiditis (RR, 2.05; 95% CI, 1.57-2.68; P=0.001).</p><p><strong>Conclusion: </strong>A significant number of patients will develop hypothyroidism or require thyroxine following hemithyroidectomy. An awareness of patient risk factors and postoperative thyroid function course will assist in counselling patients on their risk profile and guiding management.</p>","PeriodicalId":39048,"journal":{"name":"Thyroid Research","volume":"17 1","pages":"18"},"PeriodicalIF":1.8000,"publicationDate":"2024-07-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11229296/pdf/","citationCount":"0","resultStr":"{\"title\":\"Hypothyroidism after hemithyroidectomy: a systematic review and meta-analysis.\",\"authors\":\"Dominic Cooper, Rajneesh Kaur, Femi E Ayeni, Guy D Eslick, Senarath Edirimanne\",\"doi\":\"10.1186/s13044-024-00200-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The incidence of hypothyroidism following hemithyroidectomy and risk factors associated with its occurrence are not completely understood. This systematic review investigated the incidence and risk factors for hypothyroidism, thyroxine supplementation following hemithyroidectomy as well as the course of post-operative hypothyroidism, including the time to hypothyroidism and incidence of transient hypothyroidism.</p><p><strong>Methods: </strong>Searches were conducted in MEDLINE, EMBASE, Scopus, and Cochrane library for studies reporting the incidence of hypothyroidism or thyroxine supplementation following hemithyroidectomy.</p><p><strong>Results: </strong>Sixty-six studies were eligible for inclusion: 36 reported risk factors, and 27 reported post-operative course of hypothyroidism. Median follow-up was 25.2 months. The pooled incidence of hypothyroidism was 29% (95% CI, 25-34%; P<0.001). Transient hypothyroidism occurred in 34% of patients (95% CI, 21-47%; P<0.001). The pooled incidence of thyroxine supplementation was 23% (95% CI, 19-27%; P<0.001), overt hypothyroidism 4% (95% CI, 2-6%, P<0.001). Risk factors for development of hypothyroidism included pre-operative thyroid stimulating hormone (TSH) (WMD, 0.87; 95% CI, 0.75-0.98; P<0.001), TSH ≥ 2 mIU/L (RR, 2.87; 95% CI, 2.43-3.40; P<0.001), female sex (RR, 1.19; 95% CI, 1.08-1.32; P=0.007), age (WMD, 2.29; 95% CI, 1.20-3.38; P<0.001), right sided hemithyroidectomy (RR, 1.35; 95% CI, 1.10-1.65, P=0.003), the presence of autoantibodies anti-TPO (RR, 1.92; 95% CI, 1.49-2.48; P<0.001), anti-Tg (RR, 1.53; 95% CI, 1.40-1.88; P<0.001), and Hashimoto's thyroiditis (RR, 2.05; 95% CI, 1.57-2.68; P=0.001).</p><p><strong>Conclusion: </strong>A significant number of patients will develop hypothyroidism or require thyroxine following hemithyroidectomy. An awareness of patient risk factors and postoperative thyroid function course will assist in counselling patients on their risk profile and guiding management.</p>\",\"PeriodicalId\":39048,\"journal\":{\"name\":\"Thyroid Research\",\"volume\":\"17 1\",\"pages\":\"18\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-07-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11229296/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Thyroid Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13044-024-00200-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thyroid Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13044-024-00200-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Hypothyroidism after hemithyroidectomy: a systematic review and meta-analysis.
Background: The incidence of hypothyroidism following hemithyroidectomy and risk factors associated with its occurrence are not completely understood. This systematic review investigated the incidence and risk factors for hypothyroidism, thyroxine supplementation following hemithyroidectomy as well as the course of post-operative hypothyroidism, including the time to hypothyroidism and incidence of transient hypothyroidism.
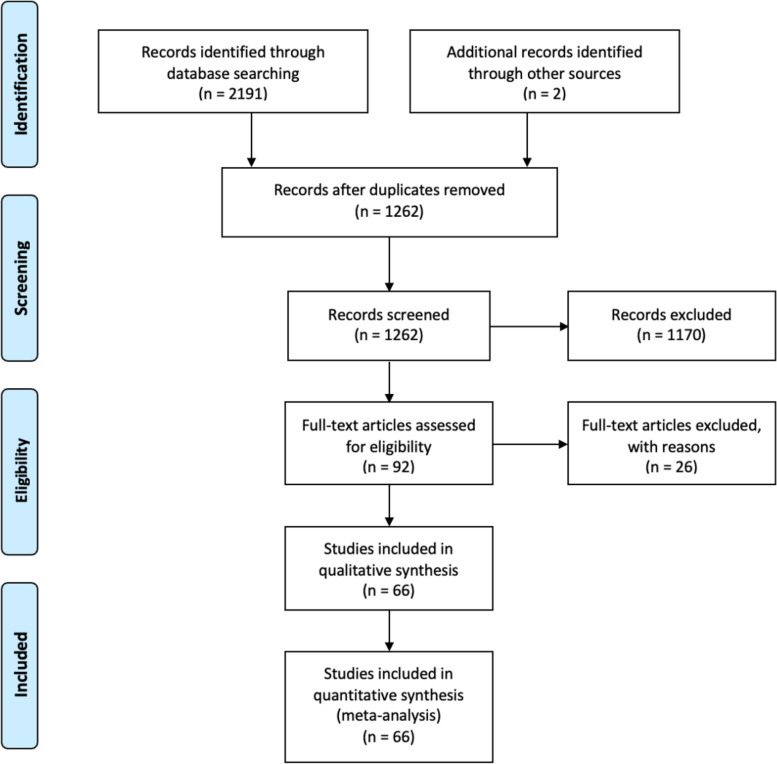
Methods: Searches were conducted in MEDLINE, EMBASE, Scopus, and Cochrane library for studies reporting the incidence of hypothyroidism or thyroxine supplementation following hemithyroidectomy.
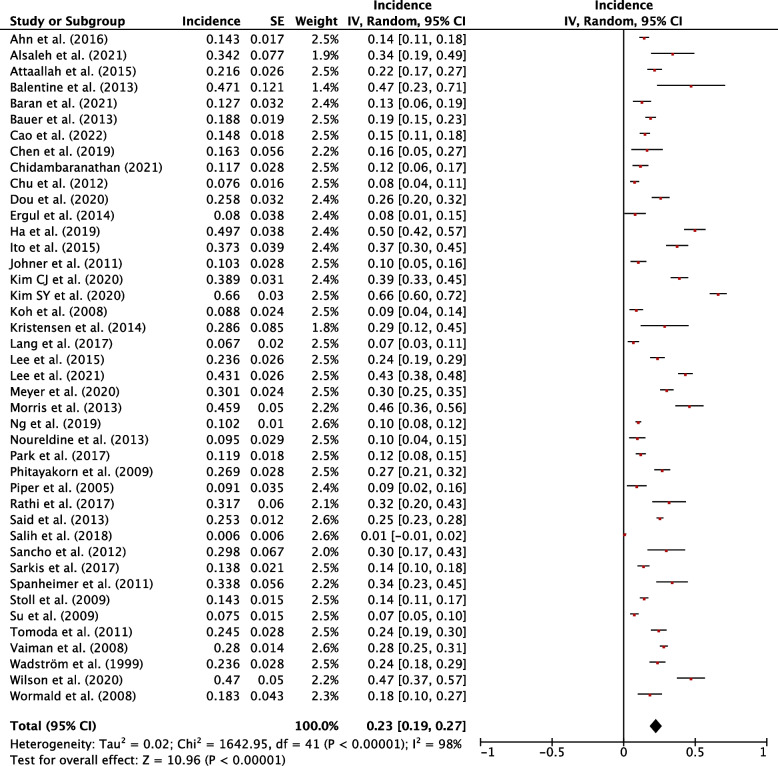
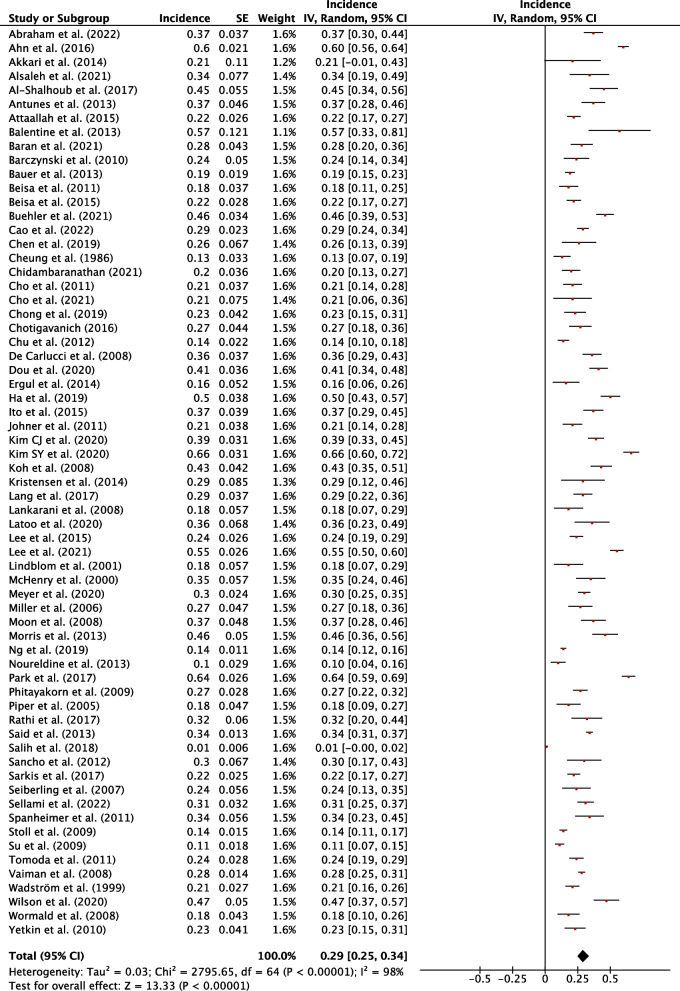
Results: Sixty-six studies were eligible for inclusion: 36 reported risk factors, and 27 reported post-operative course of hypothyroidism. Median follow-up was 25.2 months. The pooled incidence of hypothyroidism was 29% (95% CI, 25-34%; P<0.001). Transient hypothyroidism occurred in 34% of patients (95% CI, 21-47%; P<0.001). The pooled incidence of thyroxine supplementation was 23% (95% CI, 19-27%; P<0.001), overt hypothyroidism 4% (95% CI, 2-6%, P<0.001). Risk factors for development of hypothyroidism included pre-operative thyroid stimulating hormone (TSH) (WMD, 0.87; 95% CI, 0.75-0.98; P<0.001), TSH ≥ 2 mIU/L (RR, 2.87; 95% CI, 2.43-3.40; P<0.001), female sex (RR, 1.19; 95% CI, 1.08-1.32; P=0.007), age (WMD, 2.29; 95% CI, 1.20-3.38; P<0.001), right sided hemithyroidectomy (RR, 1.35; 95% CI, 1.10-1.65, P=0.003), the presence of autoantibodies anti-TPO (RR, 1.92; 95% CI, 1.49-2.48; P<0.001), anti-Tg (RR, 1.53; 95% CI, 1.40-1.88; P<0.001), and Hashimoto's thyroiditis (RR, 2.05; 95% CI, 1.57-2.68; P=0.001).
Conclusion: A significant number of patients will develop hypothyroidism or require thyroxine following hemithyroidectomy. An awareness of patient risk factors and postoperative thyroid function course will assist in counselling patients on their risk profile and guiding management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


