{"title":"准确的自我感觉健康风险是否有利于患者在发生 ST 段抬高型心肌梗死(STEMI)时尽量缩短院前延迟时间?","authors":"Karl-Heinz Ladwig, Elisabeth Olliges, Loai Albarqouni, Sophia Hoschar, Wenlin Ma, Xiaoyan Fang","doi":"10.1007/s00059-024-05256-z","DOIUrl":null,"url":null,"abstract":"<p><p>High risk perception (HRP) is fundamental for adequate health behavior. However, its impact on rapid access to cardiac care after the onset of acute myocardial infarction (AMI) is not known. Conflicting evidence exists about sources that promote HRP. Data on sociodemographic and clinical characteristics of 588 AMI patients who participated in the Munich Examination of Delay in Patients Experiencing Acute Myocardial Infarction (MEDEA) study were collected at the bedside. Adjusted multivariate logistic regression models identified factors associated with HRP. Only 13.4% (n = 79) of patients had a favorable HRP level. The HRP patients did not differ from those with low risk perception (LRP) in terms of sex, age, other sociodemographic features, and somatic risk factors. Among the univariate contributors to HRP were prodromal chest pain (p = 0.0004), symptom mismatch during AMI (p < 0.0001), depression (p = 0.01), and anxiety (p = 0.005). However, family history of AMI, a previous AMI, and knowledge of AMI remained significant in the multivariate regression model. Median delay time to reach a hospital-based emergency facility after the onset of AMI was 127 min (interquartile range [IQR]: 83-43, p = 0.02) in HRP patients and 216 min (IQR: 106-721) in LRP patients. An increasing risk perception score was associated with a corresponding stepwise decline in median delay time (p > 0.004). Self-perceived AMI risk is associated in a dose-response relationship with the time needed to reach coronary care emergency facilities. Recurrent AMI, family history of AMI, and sufficient knowledge of MI contribute to risk perception, whereas somatic risk factors do not.</p>","PeriodicalId":12863,"journal":{"name":"Herz","volume":" ","pages":"270-276"},"PeriodicalIF":0.9000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Is an accurate self-perceived health risk beneficial for patients to minimize prehospital delay time at onset of a ST-segment elevated myocardial infarction (STEMI)?\",\"authors\":\"Karl-Heinz Ladwig, Elisabeth Olliges, Loai Albarqouni, Sophia Hoschar, Wenlin Ma, Xiaoyan Fang\",\"doi\":\"10.1007/s00059-024-05256-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>High risk perception (HRP) is fundamental for adequate health behavior. However, its impact on rapid access to cardiac care after the onset of acute myocardial infarction (AMI) is not known. Conflicting evidence exists about sources that promote HRP. Data on sociodemographic and clinical characteristics of 588 AMI patients who participated in the Munich Examination of Delay in Patients Experiencing Acute Myocardial Infarction (MEDEA) study were collected at the bedside. Adjusted multivariate logistic regression models identified factors associated with HRP. Only 13.4% (n = 79) of patients had a favorable HRP level. The HRP patients did not differ from those with low risk perception (LRP) in terms of sex, age, other sociodemographic features, and somatic risk factors. Among the univariate contributors to HRP were prodromal chest pain (p = 0.0004), symptom mismatch during AMI (p < 0.0001), depression (p = 0.01), and anxiety (p = 0.005). However, family history of AMI, a previous AMI, and knowledge of AMI remained significant in the multivariate regression model. Median delay time to reach a hospital-based emergency facility after the onset of AMI was 127 min (interquartile range [IQR]: 83-43, p = 0.02) in HRP patients and 216 min (IQR: 106-721) in LRP patients. An increasing risk perception score was associated with a corresponding stepwise decline in median delay time (p > 0.004). Self-perceived AMI risk is associated in a dose-response relationship with the time needed to reach coronary care emergency facilities. Recurrent AMI, family history of AMI, and sufficient knowledge of MI contribute to risk perception, whereas somatic risk factors do not.</p>\",\"PeriodicalId\":12863,\"journal\":{\"name\":\"Herz\",\"volume\":\" \",\"pages\":\"270-276\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Herz\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00059-024-05256-z\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Herz","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00059-024-05256-z","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/4 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Is an accurate self-perceived health risk beneficial for patients to minimize prehospital delay time at onset of a ST-segment elevated myocardial infarction (STEMI)?
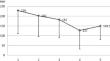
High risk perception (HRP) is fundamental for adequate health behavior. However, its impact on rapid access to cardiac care after the onset of acute myocardial infarction (AMI) is not known. Conflicting evidence exists about sources that promote HRP. Data on sociodemographic and clinical characteristics of 588 AMI patients who participated in the Munich Examination of Delay in Patients Experiencing Acute Myocardial Infarction (MEDEA) study were collected at the bedside. Adjusted multivariate logistic regression models identified factors associated with HRP. Only 13.4% (n = 79) of patients had a favorable HRP level. The HRP patients did not differ from those with low risk perception (LRP) in terms of sex, age, other sociodemographic features, and somatic risk factors. Among the univariate contributors to HRP were prodromal chest pain (p = 0.0004), symptom mismatch during AMI (p < 0.0001), depression (p = 0.01), and anxiety (p = 0.005). However, family history of AMI, a previous AMI, and knowledge of AMI remained significant in the multivariate regression model. Median delay time to reach a hospital-based emergency facility after the onset of AMI was 127 min (interquartile range [IQR]: 83-43, p = 0.02) in HRP patients and 216 min (IQR: 106-721) in LRP patients. An increasing risk perception score was associated with a corresponding stepwise decline in median delay time (p > 0.004). Self-perceived AMI risk is associated in a dose-response relationship with the time needed to reach coronary care emergency facilities. Recurrent AMI, family history of AMI, and sufficient knowledge of MI contribute to risk perception, whereas somatic risk factors do not.
期刊介绍:
Herz is the high-level journal for further education for all physicians interested in cardiology. The individual issues of the journal each deal with specific topics and comprise review articles in English and German written by competent and esteemed authors. They provide up-to-date and comprehensive information concerning the speciality dealt with in the issue. Due to the fact that all relevant aspects of the pertinent topic of an issue are considered, an overview of the current status and progress in cardiology is presented. Reviews and original articles round off the spectrum of information provided.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


