Hallie C Prescott, Megan Heath, Elizabeth S Munroe, John Blamoun, Paul Bozyk, Rachel K Hechtman, Jennifer K Horowitz, Namita Jayaprakash, Keith E Kocher, Mariam Younas, Stephanie P Taylor, Patricia J Posa, Elizabeth McLaughlin, Scott A Flanders
{"title":"开发和验证 HMS-Sepsis 死亡率模型。","authors":"Hallie C Prescott, Megan Heath, Elizabeth S Munroe, John Blamoun, Paul Bozyk, Rachel K Hechtman, Jennifer K Horowitz, Namita Jayaprakash, Keith E Kocher, Mariam Younas, Stephanie P Taylor, Patricia J Posa, Elizabeth McLaughlin, Scott A Flanders","doi":"10.1016/j.chest.2024.06.3769","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>When comparing outcomes after sepsis, it is essential to account for patient case mix to make fair comparisons. We developed a model to assess risk-adjusted 30-day mortality in the Michigan Hospital Medicine Safety sepsis initiative (HMS-Sepsis).</p><p><strong>Research question: </strong>Can HMS-Sepsis registry data adequately predict risk of 30-day mortality? Do performance assessments using adjusted vs unadjusted data differ?</p><p><strong>Study design and methods: </strong>Retrospective cohort of community-onset sepsis hospitalizations in the HMS-Sepsis registry (April 2022-September 2023), with split derivation (70%) and validation (30%) cohorts. We fit a risk-adjustment model (HMS-Sepsis mortality model) incorporating acute physiologic, demographic, and baseline health data and assessed model performance using concordance (C) statistics, Brier scores, and comparisons of predicted vs observed mortality by deciles of risk. We compared hospital performance (first quintile, middle quintiles, fifth quintile) using observed vs adjusted mortality to understand the extent to which risk adjustment impacted hospital performance assessment.</p><p><strong>Results: </strong>Among 17,514 hospitalizations from 66 hospitals during the study period, 12,260 hospitalizations (70%) were used for model derivation and 5,254 hospitalizations (30%) were used for model validation. Thirty-day mortality for the total cohort was 19.4%. The final model included 13 physiologic variables, two physiologic interactions, and 16 demographic and chronic health variables. The most significant variables were age, metastatic solid tumor, temperature, altered mental status, and platelet count. The model C statistic was 0.82 for the derivation cohort, 0.81 for the validation cohort, and ≥ 0.78 for all subgroups assessed. Overall calibration error was 0.0%, and mean calibration error across deciles of risk was 1.5%. Standardized mortality ratios yielded different assessments than observed mortality for 33.9% of hospitals.</p><p><strong>Interpretation: </strong>The HMS-Sepsis mortality model showed strong discrimination and adequate calibration and reclassified one-third of hospitals to a different performance category from unadjusted mortality. Based on its strong performance, the HMS-Sepsis mortality model may aid in fair hospital benchmarking, assessment of temporal changes, and observational causal inference analysis.</p>","PeriodicalId":9782,"journal":{"name":"Chest","volume":" ","pages":"1035-1045"},"PeriodicalIF":8.6000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11638544/pdf/","citationCount":"0","resultStr":"{\"title\":\"Development and Validation of the Hospital Medicine Safety Sepsis Initiative Mortality Model.\",\"authors\":\"Hallie C Prescott, Megan Heath, Elizabeth S Munroe, John Blamoun, Paul Bozyk, Rachel K Hechtman, Jennifer K Horowitz, Namita Jayaprakash, Keith E Kocher, Mariam Younas, Stephanie P Taylor, Patricia J Posa, Elizabeth McLaughlin, Scott A Flanders\",\"doi\":\"10.1016/j.chest.2024.06.3769\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>When comparing outcomes after sepsis, it is essential to account for patient case mix to make fair comparisons. We developed a model to assess risk-adjusted 30-day mortality in the Michigan Hospital Medicine Safety sepsis initiative (HMS-Sepsis).</p><p><strong>Research question: </strong>Can HMS-Sepsis registry data adequately predict risk of 30-day mortality? Do performance assessments using adjusted vs unadjusted data differ?</p><p><strong>Study design and methods: </strong>Retrospective cohort of community-onset sepsis hospitalizations in the HMS-Sepsis registry (April 2022-September 2023), with split derivation (70%) and validation (30%) cohorts. We fit a risk-adjustment model (HMS-Sepsis mortality model) incorporating acute physiologic, demographic, and baseline health data and assessed model performance using concordance (C) statistics, Brier scores, and comparisons of predicted vs observed mortality by deciles of risk. We compared hospital performance (first quintile, middle quintiles, fifth quintile) using observed vs adjusted mortality to understand the extent to which risk adjustment impacted hospital performance assessment.</p><p><strong>Results: </strong>Among 17,514 hospitalizations from 66 hospitals during the study period, 12,260 hospitalizations (70%) were used for model derivation and 5,254 hospitalizations (30%) were used for model validation. Thirty-day mortality for the total cohort was 19.4%. The final model included 13 physiologic variables, two physiologic interactions, and 16 demographic and chronic health variables. The most significant variables were age, metastatic solid tumor, temperature, altered mental status, and platelet count. The model C statistic was 0.82 for the derivation cohort, 0.81 for the validation cohort, and ≥ 0.78 for all subgroups assessed. Overall calibration error was 0.0%, and mean calibration error across deciles of risk was 1.5%. Standardized mortality ratios yielded different assessments than observed mortality for 33.9% of hospitals.</p><p><strong>Interpretation: </strong>The HMS-Sepsis mortality model showed strong discrimination and adequate calibration and reclassified one-third of hospitals to a different performance category from unadjusted mortality. Based on its strong performance, the HMS-Sepsis mortality model may aid in fair hospital benchmarking, assessment of temporal changes, and observational causal inference analysis.</p>\",\"PeriodicalId\":9782,\"journal\":{\"name\":\"Chest\",\"volume\":\" \",\"pages\":\"1035-1045\"},\"PeriodicalIF\":8.6000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11638544/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Chest\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1016/j.chest.2024.06.3769\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chest","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.chest.2024.06.3769","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/2 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Development and Validation of the Hospital Medicine Safety Sepsis Initiative Mortality Model.
Background: When comparing outcomes after sepsis, it is essential to account for patient case mix to make fair comparisons. We developed a model to assess risk-adjusted 30-day mortality in the Michigan Hospital Medicine Safety sepsis initiative (HMS-Sepsis).
Research question: Can HMS-Sepsis registry data adequately predict risk of 30-day mortality? Do performance assessments using adjusted vs unadjusted data differ?
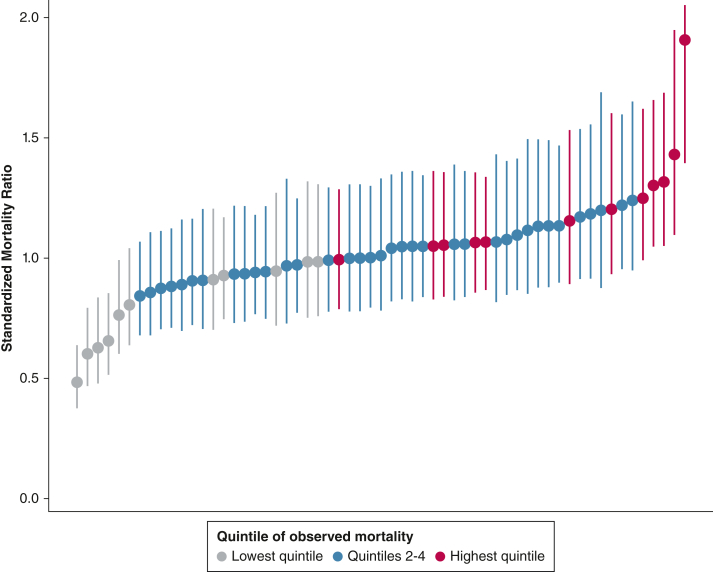
Study design and methods: Retrospective cohort of community-onset sepsis hospitalizations in the HMS-Sepsis registry (April 2022-September 2023), with split derivation (70%) and validation (30%) cohorts. We fit a risk-adjustment model (HMS-Sepsis mortality model) incorporating acute physiologic, demographic, and baseline health data and assessed model performance using concordance (C) statistics, Brier scores, and comparisons of predicted vs observed mortality by deciles of risk. We compared hospital performance (first quintile, middle quintiles, fifth quintile) using observed vs adjusted mortality to understand the extent to which risk adjustment impacted hospital performance assessment.
Results: Among 17,514 hospitalizations from 66 hospitals during the study period, 12,260 hospitalizations (70%) were used for model derivation and 5,254 hospitalizations (30%) were used for model validation. Thirty-day mortality for the total cohort was 19.4%. The final model included 13 physiologic variables, two physiologic interactions, and 16 demographic and chronic health variables. The most significant variables were age, metastatic solid tumor, temperature, altered mental status, and platelet count. The model C statistic was 0.82 for the derivation cohort, 0.81 for the validation cohort, and ≥ 0.78 for all subgroups assessed. Overall calibration error was 0.0%, and mean calibration error across deciles of risk was 1.5%. Standardized mortality ratios yielded different assessments than observed mortality for 33.9% of hospitals.
Interpretation: The HMS-Sepsis mortality model showed strong discrimination and adequate calibration and reclassified one-third of hospitals to a different performance category from unadjusted mortality. Based on its strong performance, the HMS-Sepsis mortality model may aid in fair hospital benchmarking, assessment of temporal changes, and observational causal inference analysis.
期刊介绍:
At CHEST, our mission is to revolutionize patient care through the collaboration of multidisciplinary clinicians in the fields of pulmonary, critical care, and sleep medicine. We achieve this by publishing cutting-edge clinical research that addresses current challenges and brings forth future advancements. To enhance understanding in a rapidly evolving field, CHEST also features review articles, commentaries, and facilitates discussions on emerging controversies. We place great emphasis on scientific rigor, employing a rigorous peer review process, and ensuring all accepted content is published online within two weeks.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


