Xiuyun Liu, Xinyang Liu, Huijie Yu, Kuo Zhang, Fang Guo, Mingxue Li, Shaobo Hao, Dong Ming
{"title":"一名因侧脑室颞角增宽而导致脑积水的男性患者的多模式诊断方法:病例报告","authors":"Xiuyun Liu, Xinyang Liu, Huijie Yu, Kuo Zhang, Fang Guo, Mingxue Li, Shaobo Hao, Dong Ming","doi":"10.1002/brx2.63","DOIUrl":null,"url":null,"abstract":"<p>Idiopathic normal pressure hydrocephalus (iNPH) is a disease caused by the accumulation of cerebrospinal fluid, leading to ventricular enlargement and manifesting as gait disorders, cognitive impairment, and urinary incontinence. The current diagnostic methods mainly rely on the patient's clinical symptoms, cerebrospinal fluid drainage response, and imaging results. A definitive diagnosis is suggested by significant symptom improvement post-drainage or when imaging shows an Evan's index (EI) > 0.3. Although these diagnostic methods have been widely used for many years, misdiagnoses still occur. Therefore, multimodal approaches are crucial for accurate diagnosis and treatment in complex cases. This paper reports a case of iNPH with an EI < 0.3 but with increased temporal angle width and pronounced clinical symptoms.</p><p>A 68-year-old male patient was admitted to the Tianjin Medical University General Hospital (Tianjin, China) with progressive unbalanced gait, leg weakness, urinary incontinence, and memory decline. One year ago, he underwent a head magnetic resonance imaging (MRI) at a local hospital due to trembling hands and changes in temperament; the result showed no abnormalities. Following a fall 1 month ago, he was readmitted to the same hospital for a cervical vertebra MRI examination, but no treatment was prescribed. More recently, his symptoms deteriorated, and he was admitted to our hospital for further diagnosis and treatment. He had no history of hypertension, diabetes, or coronary heart disease. On the day of his admission, the doctors arranged for an MRI, a tap test, and an infusion study due to suspected iNPH.</p><p>As shown in Figure 1, the MRI results allow for the calculation of several parameters for diagnosing iNPH, including EI, z-Evans index (z-EI), Brain/Ventricle Ratio (BVR), Corpus Callosum Angle (CA), and disproportionate enlargement of the subarachnoid space (DESH). According to current diagnostic criteria, an EI value ≥ 0.3 is an important indicator of ventricular dilation (Figure 1A).<span><sup>1</sup></span> In cases where EI < 0.3, a z-EI > 0.42 or a BVR < 1 also suggests ventricular dilation. The presence of DESH indicates a high likelihood of iNPH (Figure 1C).<span><sup>1</sup></span> In addition, a CA value < 90° suggests iNPH (Figure 1B).<span><sup>2</sup></span> In this reported case, the EI, z-EI, BVR, and CA did not meet the diagnostic criteria for iNPH, and there were no obvious DESH signs on the MRI. However, the patient's temporal horns of the lateral ventricles were significantly widened, and he demonstrated significant clinical symptoms of iNPH.</p><p>We conducted a CSF tap test (CSF-TT) and an infusion study (CSF-IT) to assess the CSF fluid circulation pathway. The CSF-TT is considered a simple, safe, and effective clinical tool for diagnosing iNPH in patients.<span><sup>3</sup></span> During the procedure, 30–50 mL of CSF is released through a lumbar puncture. We then evaluate whether there is a significant improvement in the patient's gait balance, bladder function, and advanced cognitive function 24, 48, and 72 h after the CSF drainage. As shown in Table S1, the duration and step number in the 10-m walk test improved by 11.1% and 17.6%, respectively, after CSF release. The MMSE score increased by three points, and the ICIQ score improved by more than one point. The tap test results met the diagnostic criteria for hydrocephalus.</p><p>The infusion study is a well-defined method to assess the effectiveness and necessity of proceeding with a shunt for iNPH patients.<span><sup>4</sup></span> During the infusion experiment, a sensor connected to the lumbar puncture needle monitors the patient's intracranial pressure. Meanwhile, saline is infused into the lumbar space through a micropump at a rate of 1.0 mL/min until the intracranial pressure reaches a plateau. The patient's CSF outflow resistance is then calculated by analyzing the volume-pressure curve of this process.<span><sup>4, 5</sup></span> As shown in Figure 1, the patient's opening pressure was 10.5mmHg, and the CSF outflow resistance was 12.75 mmHg*min/mL, approaching the diagnostic upper limit for iNPH.<span><sup>5</sup></span></p><p>Based on the above results, the patient was diagnosed with iNPH and recommended for ventricular-peritoneal (V-P) shunt surgery. This surgery utilized electromagnetic navigation technology to develop a navigation plan, set the target puncture point, and determine the drainage tube insertion path. This operation went smoothly, and the patient did not experience any adverse reactions. Following the surgery, the patient experienced significant improvement in symptoms.</p><p>Diagnosing iNPH precisely is always challenging. The diagnostic guidelines for hydrocephalus emphasize that MRI indicators such as the EI are beneficial for identifying patients with iNPH. However, in this case, the EI, z-EI, BVR, and CA did not meet the standard criteria of iNPH. The only significant finding was an increased temporal angle of the lateral ventricle. Given the patient's apparent clinical symptoms, we conducted multimodal diagnostic approaches.</p><p>In conclusion, although EI, DESH, and CA are considered gold-standard imaging indicators for iNPH, multimodal diagnostic approaches provide significant advantages in diagnosing and treating complex cases.</p><p><b>Xiuyun Liu</b>: Conceptualization; formal analysis; supervision; writing - review and editing. <b>Xinyang Liu</b>: Data curation; formal analysis; writing—original draft; writing - review and editing. <b>Huijie Yu</b>: Conceptualization; formal analysis; supervision; writing - review and editing. <b>Kuo Zhang</b>: Investigation; validation; writing—review and editing. <b>Fang Guo</b>: Data curation; writing—review and editing. <b>Mingxue Li</b>: Data curation; writing—review and editing. <b>Shaobo Hao</b>: Data curation; writing—review and editing. <b>Dong Ming</b>: Conceptualization; writing—review and editing.</p><p>The authors declare no conflicts of interest.</p><p>The study was approved by Ethics Committee of Tianjin Medical University General Hospital (IRB2024-YX-083-01). The patient signed the consent form and agreed to participate in this study.</p>","PeriodicalId":94303,"journal":{"name":"Brain-X","volume":"2 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-06-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/brx2.63","citationCount":"0","resultStr":"{\"title\":\"Multimodal diagnostic approaches in a male patient with hydrocephalus indicated by widening of the temporal horns of the lateral ventricles: A case report\",\"authors\":\"Xiuyun Liu, Xinyang Liu, Huijie Yu, Kuo Zhang, Fang Guo, Mingxue Li, Shaobo Hao, Dong Ming\",\"doi\":\"10.1002/brx2.63\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Idiopathic normal pressure hydrocephalus (iNPH) is a disease caused by the accumulation of cerebrospinal fluid, leading to ventricular enlargement and manifesting as gait disorders, cognitive impairment, and urinary incontinence. The current diagnostic methods mainly rely on the patient's clinical symptoms, cerebrospinal fluid drainage response, and imaging results. A definitive diagnosis is suggested by significant symptom improvement post-drainage or when imaging shows an Evan's index (EI) > 0.3. Although these diagnostic methods have been widely used for many years, misdiagnoses still occur. Therefore, multimodal approaches are crucial for accurate diagnosis and treatment in complex cases. This paper reports a case of iNPH with an EI < 0.3 but with increased temporal angle width and pronounced clinical symptoms.</p><p>A 68-year-old male patient was admitted to the Tianjin Medical University General Hospital (Tianjin, China) with progressive unbalanced gait, leg weakness, urinary incontinence, and memory decline. One year ago, he underwent a head magnetic resonance imaging (MRI) at a local hospital due to trembling hands and changes in temperament; the result showed no abnormalities. Following a fall 1 month ago, he was readmitted to the same hospital for a cervical vertebra MRI examination, but no treatment was prescribed. More recently, his symptoms deteriorated, and he was admitted to our hospital for further diagnosis and treatment. He had no history of hypertension, diabetes, or coronary heart disease. On the day of his admission, the doctors arranged for an MRI, a tap test, and an infusion study due to suspected iNPH.</p><p>As shown in Figure 1, the MRI results allow for the calculation of several parameters for diagnosing iNPH, including EI, z-Evans index (z-EI), Brain/Ventricle Ratio (BVR), Corpus Callosum Angle (CA), and disproportionate enlargement of the subarachnoid space (DESH). According to current diagnostic criteria, an EI value ≥ 0.3 is an important indicator of ventricular dilation (Figure 1A).<span><sup>1</sup></span> In cases where EI < 0.3, a z-EI > 0.42 or a BVR < 1 also suggests ventricular dilation. The presence of DESH indicates a high likelihood of iNPH (Figure 1C).<span><sup>1</sup></span> In addition, a CA value < 90° suggests iNPH (Figure 1B).<span><sup>2</sup></span> In this reported case, the EI, z-EI, BVR, and CA did not meet the diagnostic criteria for iNPH, and there were no obvious DESH signs on the MRI. However, the patient's temporal horns of the lateral ventricles were significantly widened, and he demonstrated significant clinical symptoms of iNPH.</p><p>We conducted a CSF tap test (CSF-TT) and an infusion study (CSF-IT) to assess the CSF fluid circulation pathway. The CSF-TT is considered a simple, safe, and effective clinical tool for diagnosing iNPH in patients.<span><sup>3</sup></span> During the procedure, 30–50 mL of CSF is released through a lumbar puncture. We then evaluate whether there is a significant improvement in the patient's gait balance, bladder function, and advanced cognitive function 24, 48, and 72 h after the CSF drainage. As shown in Table S1, the duration and step number in the 10-m walk test improved by 11.1% and 17.6%, respectively, after CSF release. The MMSE score increased by three points, and the ICIQ score improved by more than one point. The tap test results met the diagnostic criteria for hydrocephalus.</p><p>The infusion study is a well-defined method to assess the effectiveness and necessity of proceeding with a shunt for iNPH patients.<span><sup>4</sup></span> During the infusion experiment, a sensor connected to the lumbar puncture needle monitors the patient's intracranial pressure. Meanwhile, saline is infused into the lumbar space through a micropump at a rate of 1.0 mL/min until the intracranial pressure reaches a plateau. The patient's CSF outflow resistance is then calculated by analyzing the volume-pressure curve of this process.<span><sup>4, 5</sup></span> As shown in Figure 1, the patient's opening pressure was 10.5mmHg, and the CSF outflow resistance was 12.75 mmHg*min/mL, approaching the diagnostic upper limit for iNPH.<span><sup>5</sup></span></p><p>Based on the above results, the patient was diagnosed with iNPH and recommended for ventricular-peritoneal (V-P) shunt surgery. This surgery utilized electromagnetic navigation technology to develop a navigation plan, set the target puncture point, and determine the drainage tube insertion path. This operation went smoothly, and the patient did not experience any adverse reactions. Following the surgery, the patient experienced significant improvement in symptoms.</p><p>Diagnosing iNPH precisely is always challenging. The diagnostic guidelines for hydrocephalus emphasize that MRI indicators such as the EI are beneficial for identifying patients with iNPH. However, in this case, the EI, z-EI, BVR, and CA did not meet the standard criteria of iNPH. The only significant finding was an increased temporal angle of the lateral ventricle. Given the patient's apparent clinical symptoms, we conducted multimodal diagnostic approaches.</p><p>In conclusion, although EI, DESH, and CA are considered gold-standard imaging indicators for iNPH, multimodal diagnostic approaches provide significant advantages in diagnosing and treating complex cases.</p><p><b>Xiuyun Liu</b>: Conceptualization; formal analysis; supervision; writing - review and editing. <b>Xinyang Liu</b>: Data curation; formal analysis; writing—original draft; writing - review and editing. <b>Huijie Yu</b>: Conceptualization; formal analysis; supervision; writing - review and editing. <b>Kuo Zhang</b>: Investigation; validation; writing—review and editing. <b>Fang Guo</b>: Data curation; writing—review and editing. <b>Mingxue Li</b>: Data curation; writing—review and editing. <b>Shaobo Hao</b>: Data curation; writing—review and editing. <b>Dong Ming</b>: Conceptualization; writing—review and editing.</p><p>The authors declare no conflicts of interest.</p><p>The study was approved by Ethics Committee of Tianjin Medical University General Hospital (IRB2024-YX-083-01). The patient signed the consent form and agreed to participate in this study.</p>\",\"PeriodicalId\":94303,\"journal\":{\"name\":\"Brain-X\",\"volume\":\"2 2\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-06-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/brx2.63\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Brain-X\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/brx2.63\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain-X","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/brx2.63","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Multimodal diagnostic approaches in a male patient with hydrocephalus indicated by widening of the temporal horns of the lateral ventricles: A case report
Idiopathic normal pressure hydrocephalus (iNPH) is a disease caused by the accumulation of cerebrospinal fluid, leading to ventricular enlargement and manifesting as gait disorders, cognitive impairment, and urinary incontinence. The current diagnostic methods mainly rely on the patient's clinical symptoms, cerebrospinal fluid drainage response, and imaging results. A definitive diagnosis is suggested by significant symptom improvement post-drainage or when imaging shows an Evan's index (EI) > 0.3. Although these diagnostic methods have been widely used for many years, misdiagnoses still occur. Therefore, multimodal approaches are crucial for accurate diagnosis and treatment in complex cases. This paper reports a case of iNPH with an EI < 0.3 but with increased temporal angle width and pronounced clinical symptoms.
A 68-year-old male patient was admitted to the Tianjin Medical University General Hospital (Tianjin, China) with progressive unbalanced gait, leg weakness, urinary incontinence, and memory decline. One year ago, he underwent a head magnetic resonance imaging (MRI) at a local hospital due to trembling hands and changes in temperament; the result showed no abnormalities. Following a fall 1 month ago, he was readmitted to the same hospital for a cervical vertebra MRI examination, but no treatment was prescribed. More recently, his symptoms deteriorated, and he was admitted to our hospital for further diagnosis and treatment. He had no history of hypertension, diabetes, or coronary heart disease. On the day of his admission, the doctors arranged for an MRI, a tap test, and an infusion study due to suspected iNPH.
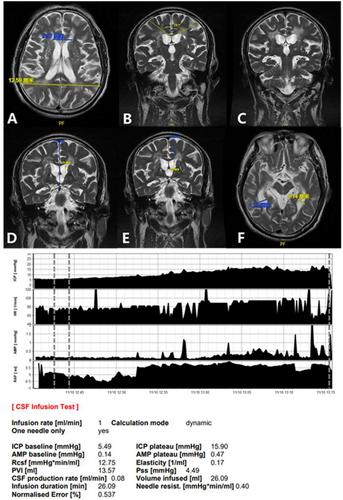
As shown in Figure 1, the MRI results allow for the calculation of several parameters for diagnosing iNPH, including EI, z-Evans index (z-EI), Brain/Ventricle Ratio (BVR), Corpus Callosum Angle (CA), and disproportionate enlargement of the subarachnoid space (DESH). According to current diagnostic criteria, an EI value ≥ 0.3 is an important indicator of ventricular dilation (Figure 1A).1 In cases where EI < 0.3, a z-EI > 0.42 or a BVR < 1 also suggests ventricular dilation. The presence of DESH indicates a high likelihood of iNPH (Figure 1C).1 In addition, a CA value < 90° suggests iNPH (Figure 1B).2 In this reported case, the EI, z-EI, BVR, and CA did not meet the diagnostic criteria for iNPH, and there were no obvious DESH signs on the MRI. However, the patient's temporal horns of the lateral ventricles were significantly widened, and he demonstrated significant clinical symptoms of iNPH.
We conducted a CSF tap test (CSF-TT) and an infusion study (CSF-IT) to assess the CSF fluid circulation pathway. The CSF-TT is considered a simple, safe, and effective clinical tool for diagnosing iNPH in patients.3 During the procedure, 30–50 mL of CSF is released through a lumbar puncture. We then evaluate whether there is a significant improvement in the patient's gait balance, bladder function, and advanced cognitive function 24, 48, and 72 h after the CSF drainage. As shown in Table S1, the duration and step number in the 10-m walk test improved by 11.1% and 17.6%, respectively, after CSF release. The MMSE score increased by three points, and the ICIQ score improved by more than one point. The tap test results met the diagnostic criteria for hydrocephalus.
The infusion study is a well-defined method to assess the effectiveness and necessity of proceeding with a shunt for iNPH patients.4 During the infusion experiment, a sensor connected to the lumbar puncture needle monitors the patient's intracranial pressure. Meanwhile, saline is infused into the lumbar space through a micropump at a rate of 1.0 mL/min until the intracranial pressure reaches a plateau. The patient's CSF outflow resistance is then calculated by analyzing the volume-pressure curve of this process.4, 5 As shown in Figure 1, the patient's opening pressure was 10.5mmHg, and the CSF outflow resistance was 12.75 mmHg*min/mL, approaching the diagnostic upper limit for iNPH.5
Based on the above results, the patient was diagnosed with iNPH and recommended for ventricular-peritoneal (V-P) shunt surgery. This surgery utilized electromagnetic navigation technology to develop a navigation plan, set the target puncture point, and determine the drainage tube insertion path. This operation went smoothly, and the patient did not experience any adverse reactions. Following the surgery, the patient experienced significant improvement in symptoms.
Diagnosing iNPH precisely is always challenging. The diagnostic guidelines for hydrocephalus emphasize that MRI indicators such as the EI are beneficial for identifying patients with iNPH. However, in this case, the EI, z-EI, BVR, and CA did not meet the standard criteria of iNPH. The only significant finding was an increased temporal angle of the lateral ventricle. Given the patient's apparent clinical symptoms, we conducted multimodal diagnostic approaches.
In conclusion, although EI, DESH, and CA are considered gold-standard imaging indicators for iNPH, multimodal diagnostic approaches provide significant advantages in diagnosing and treating complex cases.
Xiuyun Liu: Conceptualization; formal analysis; supervision; writing - review and editing. Xinyang Liu: Data curation; formal analysis; writing—original draft; writing - review and editing. Huijie Yu: Conceptualization; formal analysis; supervision; writing - review and editing. Kuo Zhang: Investigation; validation; writing—review and editing. Fang Guo: Data curation; writing—review and editing. Mingxue Li: Data curation; writing—review and editing. Shaobo Hao: Data curation; writing—review and editing. Dong Ming: Conceptualization; writing—review and editing.
The authors declare no conflicts of interest.
The study was approved by Ethics Committee of Tianjin Medical University General Hospital (IRB2024-YX-083-01). The patient signed the consent form and agreed to participate in this study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


