Katharina Mohr, Philipp Mildenberger, Thomas Neusius, Konstantinos C Christodoulou, Ioannis T Farmakis, Klaus Kaier, Stefano Barco, Frederikus A Klok, Lukas Hobohm, Karsten Keller, Dorothea Becker, Christina Abele, Leonhard Bruch, Ralf Ewert, Irene Schmidtmann, Philipp S Wild, Stephan Rosenkranz, Stavros V Konstantinides, Harald Binder, Luca Valerio
{"title":"急性肺栓塞后的年度医疗成本估算:一项前瞻性多中心队列研究的结果。","authors":"Katharina Mohr, Philipp Mildenberger, Thomas Neusius, Konstantinos C Christodoulou, Ioannis T Farmakis, Klaus Kaier, Stefano Barco, Frederikus A Klok, Lukas Hobohm, Karsten Keller, Dorothea Becker, Christina Abele, Leonhard Bruch, Ralf Ewert, Irene Schmidtmann, Philipp S Wild, Stephan Rosenkranz, Stavros V Konstantinides, Harald Binder, Luca Valerio","doi":"10.1093/ehjqcco/qcae050","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Patients surviving acute pulmonary embolism (PE) necessitate long-term treatment and follow-up. We estimated, the chronic economic impact of PE on the German healthcare system.</p><p><strong>Methods and results: </strong>We calculated the direct cost of illness during the first year after discharge for the index PE, analysing data from a multicentre prospective cohort study in Germany. Main and accompanying readmission diagnoses were used to calculate DRG-based hospital reimbursements; anticoagulation costs were estimated from the exact treatment duration and each drug's unique national identifier; and outpatient post-PE care costs from guidelines-recommended algorithms and national reimbursement catalogues. Of 1017 patients enrolled at 17 centres, 958 (94%) completed ≥3-month follow-up; of those, 24% were rehospitalized (0.34 [95% CI 0.30-0.39] readmissions per PE survivor). Age, coronary artery, pulmonary and kidney disease, diabetes, and (in the sensitivity analysis of 837 patients with complete 12-month follow-up) cancer, but not recurrent PE, were independent cost predictors by hurdle gamma regression accounting for zero readmissions. The estimated rehospitalization cost was €1138 (95% CI 896-1420) per patient. Anticoagulation duration was 329 (IQR 142-365) days, with estimated average per-patient costs of €1050 (median 972; IQR 458-1197); costs of scheduled ambulatory follow-up visits amounted to €181. Total estimated direct per-patient costs during the first year after PE ranged from €2369 (primary analysis) to €2542 (sensitivity analysis).</p><p><strong>Conclusion: </strong>By estimating per-patient costs and identifying cost drivers of post-PE care, our study may inform decisions concerning implementation and reimbursement of follow-up programmes aiming at improved cardiovascular prevention.</p>","PeriodicalId":11869,"journal":{"name":"European Heart Journal - Quality of Care and Clinical Outcomes","volume":" ","pages":"334-342"},"PeriodicalIF":4.6000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12045087/pdf/","citationCount":"0","resultStr":"{\"title\":\"Estimated annual healthcare costs after acute pulmonary embolism: results from a prospective multicentre cohort study.\",\"authors\":\"Katharina Mohr, Philipp Mildenberger, Thomas Neusius, Konstantinos C Christodoulou, Ioannis T Farmakis, Klaus Kaier, Stefano Barco, Frederikus A Klok, Lukas Hobohm, Karsten Keller, Dorothea Becker, Christina Abele, Leonhard Bruch, Ralf Ewert, Irene Schmidtmann, Philipp S Wild, Stephan Rosenkranz, Stavros V Konstantinides, Harald Binder, Luca Valerio\",\"doi\":\"10.1093/ehjqcco/qcae050\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Patients surviving acute pulmonary embolism (PE) necessitate long-term treatment and follow-up. We estimated, the chronic economic impact of PE on the German healthcare system.</p><p><strong>Methods and results: </strong>We calculated the direct cost of illness during the first year after discharge for the index PE, analysing data from a multicentre prospective cohort study in Germany. Main and accompanying readmission diagnoses were used to calculate DRG-based hospital reimbursements; anticoagulation costs were estimated from the exact treatment duration and each drug's unique national identifier; and outpatient post-PE care costs from guidelines-recommended algorithms and national reimbursement catalogues. Of 1017 patients enrolled at 17 centres, 958 (94%) completed ≥3-month follow-up; of those, 24% were rehospitalized (0.34 [95% CI 0.30-0.39] readmissions per PE survivor). Age, coronary artery, pulmonary and kidney disease, diabetes, and (in the sensitivity analysis of 837 patients with complete 12-month follow-up) cancer, but not recurrent PE, were independent cost predictors by hurdle gamma regression accounting for zero readmissions. The estimated rehospitalization cost was €1138 (95% CI 896-1420) per patient. Anticoagulation duration was 329 (IQR 142-365) days, with estimated average per-patient costs of €1050 (median 972; IQR 458-1197); costs of scheduled ambulatory follow-up visits amounted to €181. Total estimated direct per-patient costs during the first year after PE ranged from €2369 (primary analysis) to €2542 (sensitivity analysis).</p><p><strong>Conclusion: </strong>By estimating per-patient costs and identifying cost drivers of post-PE care, our study may inform decisions concerning implementation and reimbursement of follow-up programmes aiming at improved cardiovascular prevention.</p>\",\"PeriodicalId\":11869,\"journal\":{\"name\":\"European Heart Journal - Quality of Care and Clinical Outcomes\",\"volume\":\" \",\"pages\":\"334-342\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12045087/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Heart Journal - Quality of Care and Clinical Outcomes\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjqcco/qcae050\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal - Quality of Care and Clinical Outcomes","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjqcco/qcae050","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Estimated annual healthcare costs after acute pulmonary embolism: results from a prospective multicentre cohort study.
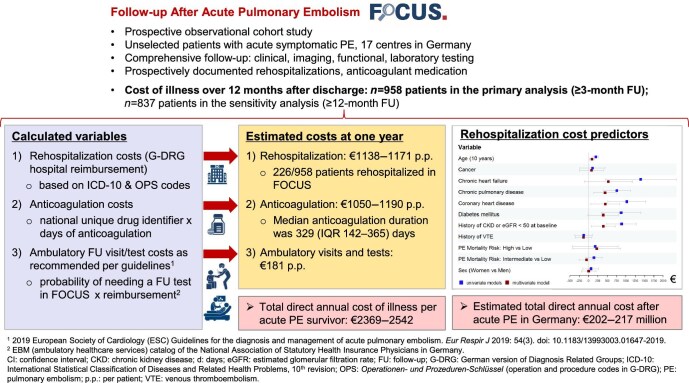
Aims: Patients surviving acute pulmonary embolism (PE) necessitate long-term treatment and follow-up. We estimated, the chronic economic impact of PE on the German healthcare system.
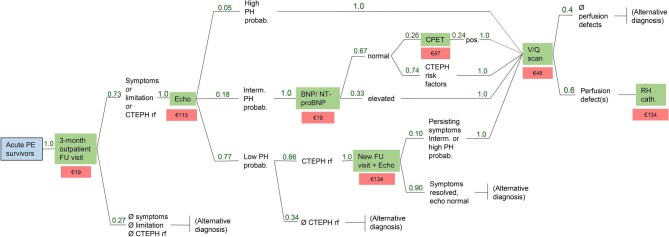
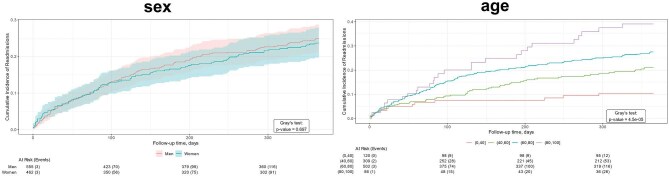
Methods and results: We calculated the direct cost of illness during the first year after discharge for the index PE, analysing data from a multicentre prospective cohort study in Germany. Main and accompanying readmission diagnoses were used to calculate DRG-based hospital reimbursements; anticoagulation costs were estimated from the exact treatment duration and each drug's unique national identifier; and outpatient post-PE care costs from guidelines-recommended algorithms and national reimbursement catalogues. Of 1017 patients enrolled at 17 centres, 958 (94%) completed ≥3-month follow-up; of those, 24% were rehospitalized (0.34 [95% CI 0.30-0.39] readmissions per PE survivor). Age, coronary artery, pulmonary and kidney disease, diabetes, and (in the sensitivity analysis of 837 patients with complete 12-month follow-up) cancer, but not recurrent PE, were independent cost predictors by hurdle gamma regression accounting for zero readmissions. The estimated rehospitalization cost was €1138 (95% CI 896-1420) per patient. Anticoagulation duration was 329 (IQR 142-365) days, with estimated average per-patient costs of €1050 (median 972; IQR 458-1197); costs of scheduled ambulatory follow-up visits amounted to €181. Total estimated direct per-patient costs during the first year after PE ranged from €2369 (primary analysis) to €2542 (sensitivity analysis).
Conclusion: By estimating per-patient costs and identifying cost drivers of post-PE care, our study may inform decisions concerning implementation and reimbursement of follow-up programmes aiming at improved cardiovascular prevention.
期刊介绍:
European Heart Journal - Quality of Care & Clinical Outcomes is an English language, peer-reviewed journal dedicated to publishing cardiovascular outcomes research. It serves as an official journal of the European Society of Cardiology and maintains a close alliance with the European Heart Health Institute. The journal disseminates original research and topical reviews contributed by health scientists globally, with a focus on the quality of care and its impact on cardiovascular outcomes at the hospital, national, and international levels. It provides a platform for presenting the most outstanding cardiovascular outcomes research to influence cardiovascular public health policy on a global scale. Additionally, the journal aims to motivate young investigators and foster the growth of the outcomes research community.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


