Francisca Castro Mendes, Vanessa Garcia-Larsen, André Moreira
{"title":"肥胖与哮喘:实施可治疗特质护理模式。","authors":"Francisca Castro Mendes, Vanessa Garcia-Larsen, André Moreira","doi":"10.1111/cea.14520","DOIUrl":null,"url":null,"abstract":"<div>\n \n <p>Recognition of obesity as a treatable trait of asthma, impacting its development, clinical presentation and management, is gaining widespread acceptance. Obesity is a significant risk factor and disease modifier for asthma, complicating treatment. Epidemiological evidence highlights that obese asthma correlates with poorer disease control, increased severity and persistence, compromised lung function and reduced quality of life. Various mechanisms contribute to the physiological and clinical complexities observed in individuals with obesity and asthma. These encompass different immune responses, including Type IVb, where T helper 2 cells are pivotal and driven by cytokines like interleukins 4, 5, 9 and 13, and Type IVc, characterised by T helper 17 cells and Type 3 innate lymphoid cells producing interleukin 17, which recruits neutrophils. Additionally, Type V involves immune response dysregulation with significant activation of T helper 1, 2 and 17 responses. Finally, Type VI is recognised as metabolic-induced immune dysregulation associated with obesity. Body mass index (BMI) stands out as a biomarker of a treatable trait in asthma, readily identifiable and targetable, with significant implications for disease management. There exists a notable gap in treatment options for individuals with obese asthma, where asthma management guidelines lack specificity. For example, there is currently no evidence supporting the use of incretin mimetics to improve asthma outcomes in asthmatic individuals without Type 2 diabetes mellitus (T2DM). In this review, we advocate for integrating BMI into asthma care models by establishing clear target BMI goals, promoting sustainable weight loss via healthy dietary choices and physical activity and implementing regular reassessment and referral as necessary.</p>\n </div>","PeriodicalId":10207,"journal":{"name":"Clinical and Experimental Allergy","volume":"54 11","pages":"881-894"},"PeriodicalIF":6.3000,"publicationDate":"2024-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Obesity and Asthma: Implementing a Treatable Trait Care Model\",\"authors\":\"Francisca Castro Mendes, Vanessa Garcia-Larsen, André Moreira\",\"doi\":\"10.1111/cea.14520\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n <p>Recognition of obesity as a treatable trait of asthma, impacting its development, clinical presentation and management, is gaining widespread acceptance. Obesity is a significant risk factor and disease modifier for asthma, complicating treatment. Epidemiological evidence highlights that obese asthma correlates with poorer disease control, increased severity and persistence, compromised lung function and reduced quality of life. Various mechanisms contribute to the physiological and clinical complexities observed in individuals with obesity and asthma. These encompass different immune responses, including Type IVb, where T helper 2 cells are pivotal and driven by cytokines like interleukins 4, 5, 9 and 13, and Type IVc, characterised by T helper 17 cells and Type 3 innate lymphoid cells producing interleukin 17, which recruits neutrophils. Additionally, Type V involves immune response dysregulation with significant activation of T helper 1, 2 and 17 responses. Finally, Type VI is recognised as metabolic-induced immune dysregulation associated with obesity. Body mass index (BMI) stands out as a biomarker of a treatable trait in asthma, readily identifiable and targetable, with significant implications for disease management. There exists a notable gap in treatment options for individuals with obese asthma, where asthma management guidelines lack specificity. For example, there is currently no evidence supporting the use of incretin mimetics to improve asthma outcomes in asthmatic individuals without Type 2 diabetes mellitus (T2DM). In this review, we advocate for integrating BMI into asthma care models by establishing clear target BMI goals, promoting sustainable weight loss via healthy dietary choices and physical activity and implementing regular reassessment and referral as necessary.</p>\\n </div>\",\"PeriodicalId\":10207,\"journal\":{\"name\":\"Clinical and Experimental Allergy\",\"volume\":\"54 11\",\"pages\":\"881-894\"},\"PeriodicalIF\":6.3000,\"publicationDate\":\"2024-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Allergy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/cea.14520\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cea.14520","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
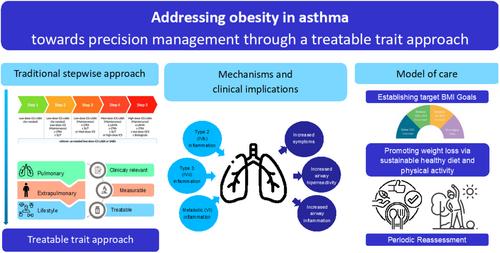
Obesity and Asthma: Implementing a Treatable Trait Care Model
Recognition of obesity as a treatable trait of asthma, impacting its development, clinical presentation and management, is gaining widespread acceptance. Obesity is a significant risk factor and disease modifier for asthma, complicating treatment. Epidemiological evidence highlights that obese asthma correlates with poorer disease control, increased severity and persistence, compromised lung function and reduced quality of life. Various mechanisms contribute to the physiological and clinical complexities observed in individuals with obesity and asthma. These encompass different immune responses, including Type IVb, where T helper 2 cells are pivotal and driven by cytokines like interleukins 4, 5, 9 and 13, and Type IVc, characterised by T helper 17 cells and Type 3 innate lymphoid cells producing interleukin 17, which recruits neutrophils. Additionally, Type V involves immune response dysregulation with significant activation of T helper 1, 2 and 17 responses. Finally, Type VI is recognised as metabolic-induced immune dysregulation associated with obesity. Body mass index (BMI) stands out as a biomarker of a treatable trait in asthma, readily identifiable and targetable, with significant implications for disease management. There exists a notable gap in treatment options for individuals with obese asthma, where asthma management guidelines lack specificity. For example, there is currently no evidence supporting the use of incretin mimetics to improve asthma outcomes in asthmatic individuals without Type 2 diabetes mellitus (T2DM). In this review, we advocate for integrating BMI into asthma care models by establishing clear target BMI goals, promoting sustainable weight loss via healthy dietary choices and physical activity and implementing regular reassessment and referral as necessary.
期刊介绍:
Clinical & Experimental Allergy strikes an excellent balance between clinical and scientific articles and carries regular reviews and editorials written by leading authorities in their field.
In response to the increasing number of quality submissions, since 1996 the journals size has increased by over 30%. Clinical & Experimental Allergy is essential reading for allergy practitioners and research scientists with an interest in allergic diseases and mechanisms. Truly international in appeal, Clinical & Experimental Allergy publishes clinical and experimental observations in disease in all fields of medicine in which allergic hypersensitivity plays a part.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


