Ester J. Herrmann, Badrinarayanan Raghavan, Meaza Tekeste, Kathleen Mantzsch, Patrick Meybohm, Birgit Assmus
{"title":"对需要进行非心脏手术的心力衰竭患者进行术前和术后护士支持护理的随机试点试验--可行性和结果。","authors":"Ester J. Herrmann, Badrinarayanan Raghavan, Meaza Tekeste, Kathleen Mantzsch, Patrick Meybohm, Birgit Assmus","doi":"10.1002/clc.24304","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>The perioperative cardiovascular management of patients undergoing noncardiac surgery is particularly challenging in those with pre-existing heart failure (HF). This study was designed to evaluate the effectiveness of nurse-based pre- and postoperative specialized HF management in reducing postoperative HF-associated complications in patients with known HF undergoing noncardiac surgery.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This prospective, randomized pilot study included patients with established HF requiring intermediate- to high-risk noncardiac surgery. Patients received postoperatively either standard care (control group, CG) or nurse-supported HF management (intervention group, IG). The primary endpoint was a composite of HF-related postoperative complications at 30 days. Secondary endpoints included length on intensive care unit, length of hospital stay, death, hospitalization for HF, and quality of life assessment using the SF-12 questionnaire.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The trial was halted prematurely for futility. A total of 34 patients (median age 70.5 [IQR 67–75] years; with 15 HfpEF, 9 HfmrEF,10 HfrEF), with an average NT-proBNP of 1.413 [463–2.832] pg/mL were included. The IG had a lower rate of postoperative primary events (25%; <i>n</i> = 4) compared with the CG (33%; <i>n</i> = 6). There were no differences in secondary endpoints between the groups. Quality-of-life scores improved slightly in both groups (<i>δ</i> 5.6 ± 0.9 [CG] and 3.1 ± 1.2 [IG]).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Nurse-based pre- and postoperative HF care appears to be feasible and may reduce HF-associated complications in patients undergoing noncardiac surgery. Larger clinical trials are needed to further evaluate the effectiveness of this approach in reducing postoperative complications in this high-risk patient population.</p>\n </section>\n </div>","PeriodicalId":10201,"journal":{"name":"Clinical Cardiology","volume":"47 6","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2024-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11194970/pdf/","citationCount":"0","resultStr":"{\"title\":\"Randomized Pilot Trial of Pre- and Postoperative Heart Failure Nurse-Supported Care in Heart Failure Patients Requiring Noncardiac Surgery—Feasibility and Results\",\"authors\":\"Ester J. Herrmann, Badrinarayanan Raghavan, Meaza Tekeste, Kathleen Mantzsch, Patrick Meybohm, Birgit Assmus\",\"doi\":\"10.1002/clc.24304\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>The perioperative cardiovascular management of patients undergoing noncardiac surgery is particularly challenging in those with pre-existing heart failure (HF). This study was designed to evaluate the effectiveness of nurse-based pre- and postoperative specialized HF management in reducing postoperative HF-associated complications in patients with known HF undergoing noncardiac surgery.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This prospective, randomized pilot study included patients with established HF requiring intermediate- to high-risk noncardiac surgery. Patients received postoperatively either standard care (control group, CG) or nurse-supported HF management (intervention group, IG). The primary endpoint was a composite of HF-related postoperative complications at 30 days. Secondary endpoints included length on intensive care unit, length of hospital stay, death, hospitalization for HF, and quality of life assessment using the SF-12 questionnaire.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The trial was halted prematurely for futility. A total of 34 patients (median age 70.5 [IQR 67–75] years; with 15 HfpEF, 9 HfmrEF,10 HfrEF), with an average NT-proBNP of 1.413 [463–2.832] pg/mL were included. The IG had a lower rate of postoperative primary events (25%; <i>n</i> = 4) compared with the CG (33%; <i>n</i> = 6). There were no differences in secondary endpoints between the groups. Quality-of-life scores improved slightly in both groups (<i>δ</i> 5.6 ± 0.9 [CG] and 3.1 ± 1.2 [IG]).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Nurse-based pre- and postoperative HF care appears to be feasible and may reduce HF-associated complications in patients undergoing noncardiac surgery. Larger clinical trials are needed to further evaluate the effectiveness of this approach in reducing postoperative complications in this high-risk patient population.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10201,\"journal\":{\"name\":\"Clinical Cardiology\",\"volume\":\"47 6\",\"pages\":\"\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-06-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11194970/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clc.24304\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Cardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.24304","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Randomized Pilot Trial of Pre- and Postoperative Heart Failure Nurse-Supported Care in Heart Failure Patients Requiring Noncardiac Surgery—Feasibility and Results
Introduction
The perioperative cardiovascular management of patients undergoing noncardiac surgery is particularly challenging in those with pre-existing heart failure (HF). This study was designed to evaluate the effectiveness of nurse-based pre- and postoperative specialized HF management in reducing postoperative HF-associated complications in patients with known HF undergoing noncardiac surgery.
Methods
This prospective, randomized pilot study included patients with established HF requiring intermediate- to high-risk noncardiac surgery. Patients received postoperatively either standard care (control group, CG) or nurse-supported HF management (intervention group, IG). The primary endpoint was a composite of HF-related postoperative complications at 30 days. Secondary endpoints included length on intensive care unit, length of hospital stay, death, hospitalization for HF, and quality of life assessment using the SF-12 questionnaire.
Results
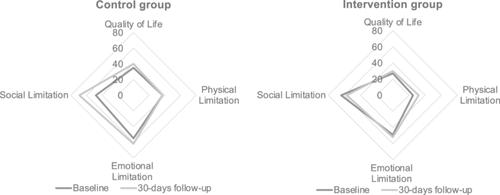
The trial was halted prematurely for futility. A total of 34 patients (median age 70.5 [IQR 67–75] years; with 15 HfpEF, 9 HfmrEF,10 HfrEF), with an average NT-proBNP of 1.413 [463–2.832] pg/mL were included. The IG had a lower rate of postoperative primary events (25%; n = 4) compared with the CG (33%; n = 6). There were no differences in secondary endpoints between the groups. Quality-of-life scores improved slightly in both groups (δ 5.6 ± 0.9 [CG] and 3.1 ± 1.2 [IG]).
Conclusion
Nurse-based pre- and postoperative HF care appears to be feasible and may reduce HF-associated complications in patients undergoing noncardiac surgery. Larger clinical trials are needed to further evaluate the effectiveness of this approach in reducing postoperative complications in this high-risk patient population.
期刊介绍:
Clinical Cardiology provides a fully Gold Open Access forum for the publication of original clinical research, as well as brief reviews of diagnostic and therapeutic issues in cardiovascular medicine and cardiovascular surgery.
The journal includes Clinical Investigations, Reviews, free standing editorials and commentaries, and bonus online-only content.
The journal also publishes supplements, Expert Panel Discussions, sponsored clinical Reviews, Trial Designs, and Quality and Outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


