{"title":"基于生理学的药代动力学模型研究 CYP3A4/3A5 成熟对儿科造血干细胞移植患者他克莫司药代动力学的影响","authors":"","doi":"10.1016/j.ejps.2024.106839","DOIUrl":null,"url":null,"abstract":"<div><p>Tacrolimus (FK506) is a cornerstone of GVHD-prophylaxis treatment in paediatrics undergoing haematopoietic stem cell transplantation (HSCT). However, due to concerns about highly inter/intra-individual variability, precision dosing of FK506 is crucial. Cytochrome P450 (CYP) 3A4 and 3A5 are considered important sources of FK506 pharmacokinetic variability. Nevertheless, the impact of age-related maturation in hepatic and intestinal CYP3A4/3A5 enzymes remains unknown in paediatric HSCT patients. Physiologically-based pharmacokinetic (PBPK) models were developed and verified in adult volunteers and adult HSCT patients using GastroPlus™ <sup>(</sup>version 9.0), and then extrapolated to paediatric HSCT patients, taking into account the maturation of CYP3A4 and CYP3A5. Default CYP3A4 and CYP3A5 ontogeny profiles were updated based on the latest reports. The paediatric PBPK model was evaluated with independent data collected from Sun Yat-sen Memorial Hospital (86 paediatric HSCT patients, 1 to 16 -year-old). Simulations were performed to evaluate a reported FK506 dosing regimen in infants and children with different CYP3A5 genotypes. Extensive PBPK model validation indicated good predictability, with the predicted/observed (P/O) ratios within the range of 0.80-fold to 1.25-fold. Blood tacrolimus concentration-time curves were comparable between the real and virtual patients. Simulations showed that the higher levels of tacrolimus in 9-month-old to 3-year-old infants were mainly attributed to the CYP3A4/3A5 ontogeny profiles, which resulted in lower clearance and higher exposure relative to dose. The oral dosage of 0.1 mg/kg/day (q12 h) is considered appropriate for paediatric HSCT patients 9 months to 15 years of age with <em>CYP3A5 *1/*1</em> genotypes. Lower doses were required for paediatric HSCT patients with <em>CYP3A5 *1/*3 (</em>0.08 mg/kg/day, q12h) or <em>CYP3A5 *3/*3</em> genotypes <em>(</em>0.07 mg/kg/day, q12h), and analyses demonstrated 12.5–20 % decreases in ≤3-year-old patients. The study highlights the feasibility of PBPK modelling to explore age-related enzyme maturation in infants and children (≤3-year-old) undergoing HSCT and emphasizes the need to include hepatic and gut CYP3A4/3A5 maturation parameters.</p></div>","PeriodicalId":12018,"journal":{"name":"European Journal of Pharmaceutical Sciences","volume":null,"pages":null},"PeriodicalIF":4.3000,"publicationDate":"2024-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S0928098724001519/pdfft?md5=a32bf0c1cb738ac0ba71510e73619e8f&pid=1-s2.0-S0928098724001519-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Physiologically-based pharmacokinetic modelling to investigate the effect of CYP3A4/3A5 maturation on tacrolimus pharmacokinetics in paediatric HSCT patients\",\"authors\":\"\",\"doi\":\"10.1016/j.ejps.2024.106839\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p>Tacrolimus (FK506) is a cornerstone of GVHD-prophylaxis treatment in paediatrics undergoing haematopoietic stem cell transplantation (HSCT). However, due to concerns about highly inter/intra-individual variability, precision dosing of FK506 is crucial. Cytochrome P450 (CYP) 3A4 and 3A5 are considered important sources of FK506 pharmacokinetic variability. Nevertheless, the impact of age-related maturation in hepatic and intestinal CYP3A4/3A5 enzymes remains unknown in paediatric HSCT patients. Physiologically-based pharmacokinetic (PBPK) models were developed and verified in adult volunteers and adult HSCT patients using GastroPlus™ <sup>(</sup>version 9.0), and then extrapolated to paediatric HSCT patients, taking into account the maturation of CYP3A4 and CYP3A5. Default CYP3A4 and CYP3A5 ontogeny profiles were updated based on the latest reports. The paediatric PBPK model was evaluated with independent data collected from Sun Yat-sen Memorial Hospital (86 paediatric HSCT patients, 1 to 16 -year-old). Simulations were performed to evaluate a reported FK506 dosing regimen in infants and children with different CYP3A5 genotypes. Extensive PBPK model validation indicated good predictability, with the predicted/observed (P/O) ratios within the range of 0.80-fold to 1.25-fold. Blood tacrolimus concentration-time curves were comparable between the real and virtual patients. Simulations showed that the higher levels of tacrolimus in 9-month-old to 3-year-old infants were mainly attributed to the CYP3A4/3A5 ontogeny profiles, which resulted in lower clearance and higher exposure relative to dose. The oral dosage of 0.1 mg/kg/day (q12 h) is considered appropriate for paediatric HSCT patients 9 months to 15 years of age with <em>CYP3A5 *1/*1</em> genotypes. Lower doses were required for paediatric HSCT patients with <em>CYP3A5 *1/*3 (</em>0.08 mg/kg/day, q12h) or <em>CYP3A5 *3/*3</em> genotypes <em>(</em>0.07 mg/kg/day, q12h), and analyses demonstrated 12.5–20 % decreases in ≤3-year-old patients. The study highlights the feasibility of PBPK modelling to explore age-related enzyme maturation in infants and children (≤3-year-old) undergoing HSCT and emphasizes the need to include hepatic and gut CYP3A4/3A5 maturation parameters.</p></div>\",\"PeriodicalId\":12018,\"journal\":{\"name\":\"European Journal of Pharmaceutical Sciences\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-06-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S0928098724001519/pdfft?md5=a32bf0c1cb738ac0ba71510e73619e8f&pid=1-s2.0-S0928098724001519-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Pharmaceutical Sciences\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0928098724001519\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Pharmaceutical Sciences","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0928098724001519","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Physiologically-based pharmacokinetic modelling to investigate the effect of CYP3A4/3A5 maturation on tacrolimus pharmacokinetics in paediatric HSCT patients
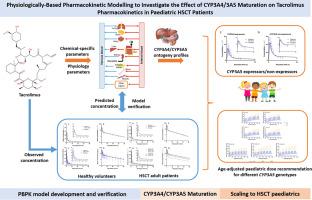
Tacrolimus (FK506) is a cornerstone of GVHD-prophylaxis treatment in paediatrics undergoing haematopoietic stem cell transplantation (HSCT). However, due to concerns about highly inter/intra-individual variability, precision dosing of FK506 is crucial. Cytochrome P450 (CYP) 3A4 and 3A5 are considered important sources of FK506 pharmacokinetic variability. Nevertheless, the impact of age-related maturation in hepatic and intestinal CYP3A4/3A5 enzymes remains unknown in paediatric HSCT patients. Physiologically-based pharmacokinetic (PBPK) models were developed and verified in adult volunteers and adult HSCT patients using GastroPlus™ (version 9.0), and then extrapolated to paediatric HSCT patients, taking into account the maturation of CYP3A4 and CYP3A5. Default CYP3A4 and CYP3A5 ontogeny profiles were updated based on the latest reports. The paediatric PBPK model was evaluated with independent data collected from Sun Yat-sen Memorial Hospital (86 paediatric HSCT patients, 1 to 16 -year-old). Simulations were performed to evaluate a reported FK506 dosing regimen in infants and children with different CYP3A5 genotypes. Extensive PBPK model validation indicated good predictability, with the predicted/observed (P/O) ratios within the range of 0.80-fold to 1.25-fold. Blood tacrolimus concentration-time curves were comparable between the real and virtual patients. Simulations showed that the higher levels of tacrolimus in 9-month-old to 3-year-old infants were mainly attributed to the CYP3A4/3A5 ontogeny profiles, which resulted in lower clearance and higher exposure relative to dose. The oral dosage of 0.1 mg/kg/day (q12 h) is considered appropriate for paediatric HSCT patients 9 months to 15 years of age with CYP3A5 *1/*1 genotypes. Lower doses were required for paediatric HSCT patients with CYP3A5 *1/*3 (0.08 mg/kg/day, q12h) or CYP3A5 *3/*3 genotypes (0.07 mg/kg/day, q12h), and analyses demonstrated 12.5–20 % decreases in ≤3-year-old patients. The study highlights the feasibility of PBPK modelling to explore age-related enzyme maturation in infants and children (≤3-year-old) undergoing HSCT and emphasizes the need to include hepatic and gut CYP3A4/3A5 maturation parameters.
期刊介绍:
The journal publishes research articles, review articles and scientific commentaries on all aspects of the pharmaceutical sciences with emphasis on conceptual novelty and scientific quality. The Editors welcome articles in this multidisciplinary field, with a focus on topics relevant for drug discovery and development.
More specifically, the Journal publishes reports on medicinal chemistry, pharmacology, drug absorption and metabolism, pharmacokinetics and pharmacodynamics, pharmaceutical and biomedical analysis, drug delivery (including gene delivery), drug targeting, pharmaceutical technology, pharmaceutical biotechnology and clinical drug evaluation. The journal will typically not give priority to manuscripts focusing primarily on organic synthesis, natural products, adaptation of analytical approaches, or discussions pertaining to drug policy making.
Scientific commentaries and review articles are generally by invitation only or by consent of the Editors. Proceedings of scientific meetings may be published as special issues or supplements to the Journal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


