Paolo Compagnucci MD, PhD , Giovanni Volpato MD , Laura Cipolletta MD, PhD , Quintino Parisi MD, PhD , Yari Valeri MD , Francesca Campanelli MD , Leonardo D’Angelo MD , Giuseppe Ciliberti MD, PhD , Giulia Stronati MD , Laura Carboni MD , Andrea Giovagnoni MD , Federico Guerra MD, FEHRA , Andrea Natale MD, FHRS , Michela Casella MD, PhD, FEHRA , Antonio Dello Russo MD, PhD
{"title":"后壁消融治疗持续性心房颤动:超高功率短时射频消融术与标准功率射频消融术的比较","authors":"Paolo Compagnucci MD, PhD , Giovanni Volpato MD , Laura Cipolletta MD, PhD , Quintino Parisi MD, PhD , Yari Valeri MD , Francesca Campanelli MD , Leonardo D’Angelo MD , Giuseppe Ciliberti MD, PhD , Giulia Stronati MD , Laura Carboni MD , Andrea Giovagnoni MD , Federico Guerra MD, FEHRA , Andrea Natale MD, FHRS , Michela Casella MD, PhD, FEHRA , Antonio Dello Russo MD, PhD","doi":"10.1016/j.hroo.2024.04.011","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Posterior wall ablation (PWA) is commonly added to pulmonary vein isolation (PVI) during catheter ablation (CA) of persistent atrial fibrillation (AF).</p></div><div><h3>Objective</h3><p>The purpose of this study was to compare PVI plus PWA using very-high-power short-duration (vHPSD) vs standard-power (SP) ablation index-guided CA among consecutive patients with persistent AF and to determine the voltage correlation between microbipolar and bipolar mapping in AF.</p></div><div><h3>Methods</h3><p>We compared 40 patients undergoing PVI plus PWA using vHPSD to 40 controls receiving PVI plus PWA using SP. The primary efficacy endpoint was recurrence of atrial tachyarrhythmias after a 3-month blanking period. The primary safety outcome was a composite of major complications within 30 days after CA. In the vHPSD group, high-density mapping of the posterior wall was performed using both a multipolar catheter and microelectrodes on the tip of the ablation catheter.</p></div><div><h3>Results</h3><p>PVI was more commonly obtained with vHPSD compared to SP ablation (98%vs 75%; <em>P</em> = .007), despite shorter procedural and fluoroscopy times (<em>P</em> <.001). Survival free from recurrent atrial tachyarrhythmias at 18 months was 68% and 47% in the vHPSD and SP groups, respectively (log-rank <em>P</em> = .071), without major adverse events. The vHPSD approach was significantly associated with reduced risk of recurrent AF at multivariable analysis (hazard ratio 0.39; <em>P</em> = .030). Microbipolar voltage cutoffs of 0.71 and 1.69 mV predicted minimum bipolar values of 0.16 and 0.31 mV in AF, respectively, with accuracies of 0.67 and 0.88.</p></div><div><h3>Conclusion</h3><p>vHPSD PWA plus PVI may be faster and as safe as SP CA among patients with persistent AF, with a trend for superior efficacy. Adapted voltage cutoffs should be used for identifying atrial low-voltage areas with microbipolar mapping.</p></div>","PeriodicalId":29772,"journal":{"name":"Heart Rhythm O2","volume":"5 6","pages":"Pages 374-384"},"PeriodicalIF":2.5000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2666501824001065/pdfft?md5=06d881cf35c4d69ff99c2717bf9b532b&pid=1-s2.0-S2666501824001065-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Posterior wall ablation for persistent atrial fibrillation: Very-high-power short-duration versus standard-power radiofrequency ablation\",\"authors\":\"Paolo Compagnucci MD, PhD , Giovanni Volpato MD , Laura Cipolletta MD, PhD , Quintino Parisi MD, PhD , Yari Valeri MD , Francesca Campanelli MD , Leonardo D’Angelo MD , Giuseppe Ciliberti MD, PhD , Giulia Stronati MD , Laura Carboni MD , Andrea Giovagnoni MD , Federico Guerra MD, FEHRA , Andrea Natale MD, FHRS , Michela Casella MD, PhD, FEHRA , Antonio Dello Russo MD, PhD\",\"doi\":\"10.1016/j.hroo.2024.04.011\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Posterior wall ablation (PWA) is commonly added to pulmonary vein isolation (PVI) during catheter ablation (CA) of persistent atrial fibrillation (AF).</p></div><div><h3>Objective</h3><p>The purpose of this study was to compare PVI plus PWA using very-high-power short-duration (vHPSD) vs standard-power (SP) ablation index-guided CA among consecutive patients with persistent AF and to determine the voltage correlation between microbipolar and bipolar mapping in AF.</p></div><div><h3>Methods</h3><p>We compared 40 patients undergoing PVI plus PWA using vHPSD to 40 controls receiving PVI plus PWA using SP. The primary efficacy endpoint was recurrence of atrial tachyarrhythmias after a 3-month blanking period. The primary safety outcome was a composite of major complications within 30 days after CA. In the vHPSD group, high-density mapping of the posterior wall was performed using both a multipolar catheter and microelectrodes on the tip of the ablation catheter.</p></div><div><h3>Results</h3><p>PVI was more commonly obtained with vHPSD compared to SP ablation (98%vs 75%; <em>P</em> = .007), despite shorter procedural and fluoroscopy times (<em>P</em> <.001). Survival free from recurrent atrial tachyarrhythmias at 18 months was 68% and 47% in the vHPSD and SP groups, respectively (log-rank <em>P</em> = .071), without major adverse events. The vHPSD approach was significantly associated with reduced risk of recurrent AF at multivariable analysis (hazard ratio 0.39; <em>P</em> = .030). Microbipolar voltage cutoffs of 0.71 and 1.69 mV predicted minimum bipolar values of 0.16 and 0.31 mV in AF, respectively, with accuracies of 0.67 and 0.88.</p></div><div><h3>Conclusion</h3><p>vHPSD PWA plus PVI may be faster and as safe as SP CA among patients with persistent AF, with a trend for superior efficacy. Adapted voltage cutoffs should be used for identifying atrial low-voltage areas with microbipolar mapping.</p></div>\",\"PeriodicalId\":29772,\"journal\":{\"name\":\"Heart Rhythm O2\",\"volume\":\"5 6\",\"pages\":\"Pages 374-384\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2666501824001065/pdfft?md5=06d881cf35c4d69ff99c2717bf9b532b&pid=1-s2.0-S2666501824001065-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Heart Rhythm O2\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666501824001065\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Heart Rhythm O2","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666501824001065","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Posterior wall ablation for persistent atrial fibrillation: Very-high-power short-duration versus standard-power radiofrequency ablation
Background
Posterior wall ablation (PWA) is commonly added to pulmonary vein isolation (PVI) during catheter ablation (CA) of persistent atrial fibrillation (AF).
Objective
The purpose of this study was to compare PVI plus PWA using very-high-power short-duration (vHPSD) vs standard-power (SP) ablation index-guided CA among consecutive patients with persistent AF and to determine the voltage correlation between microbipolar and bipolar mapping in AF.
Methods
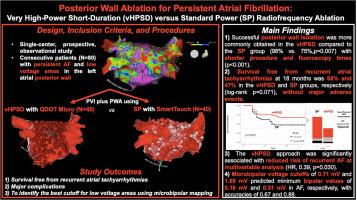
We compared 40 patients undergoing PVI plus PWA using vHPSD to 40 controls receiving PVI plus PWA using SP. The primary efficacy endpoint was recurrence of atrial tachyarrhythmias after a 3-month blanking period. The primary safety outcome was a composite of major complications within 30 days after CA. In the vHPSD group, high-density mapping of the posterior wall was performed using both a multipolar catheter and microelectrodes on the tip of the ablation catheter.
Results
PVI was more commonly obtained with vHPSD compared to SP ablation (98%vs 75%; P = .007), despite shorter procedural and fluoroscopy times (P <.001). Survival free from recurrent atrial tachyarrhythmias at 18 months was 68% and 47% in the vHPSD and SP groups, respectively (log-rank P = .071), without major adverse events. The vHPSD approach was significantly associated with reduced risk of recurrent AF at multivariable analysis (hazard ratio 0.39; P = .030). Microbipolar voltage cutoffs of 0.71 and 1.69 mV predicted minimum bipolar values of 0.16 and 0.31 mV in AF, respectively, with accuracies of 0.67 and 0.88.
Conclusion
vHPSD PWA plus PVI may be faster and as safe as SP CA among patients with persistent AF, with a trend for superior efficacy. Adapted voltage cutoffs should be used for identifying atrial low-voltage areas with microbipolar mapping.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


