{"title":"一例通过口腔直接数字胆管造影术彻底清除堆叠的胆总管结石的病例,患者因手术改变了解剖结构。","authors":"Noriyuki Hirakawa, Katsuya Kitamura, Takao Itoi","doi":"10.1002/jhbp.12013","DOIUrl":null,"url":null,"abstract":"<p>Treatment of common bile duct stones or anastomotic stenosis is challenging in patients with surgically altered anatomy (SAA). Although the clinical outcomes of balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography (BE-ERCP) have been improving in these patients,<span><sup>1-3</sup></span> stacked stones are still difficult to remove in some cases. There are also cases in which electrohydraulic lithotripsy (EHL) is required for the removal of stacked stones in patients with SAA.<span><sup>4</sup></span></p><p>The patient in this case was an 89-year-old man who had undergone Roux-en Y reconstruction after resection of gastric cancer. He was admitted to our hospital for treatment of cholangitis due to stacked common bile duct stones. BE-ERCP was attempted for bile duct drainage, but the papilla could not be identified and percutaneous transhepatic biliary drainage was performed. Then rendezvous BE-ERCP using the percutaneous transhepatic drainage route was performed (Figure 1). Although the papilla could be identified, the stacked stones were difficult to remove, and EHL was planned for the next session. Unfortunately, a peroral direct digital cholangioscope (SpyDS; Boston Scientific, Natick, Massachusetts, USA) with a caliber of 3.3 mm was not available for BE-ERCP because of the limited diameter of the accessory channel (3.2 mm). Therefore, ERCP was performed using a colonoscope (CF-XZ1200; Olympus Medical, Tokyo, Japan), in which the cholangioscope can be inserted via the accessory channel (3.7 mm).</p><p>The cholangioscope was inserted into the common bile duct via the CF-XZ1200 and showed that the common bile duct was filled with stacked stones. The stacked stones were crushed by EHL and cholangiography showed that the stones were reduced in size. The stones were completely removed using a mechanical lithotripter and basket catheter. The patient had a favorable course and was discharged (Figure 2).</p><p>This case demonstrates that stacked stones can be safely and effectively removed by EHL and other tools with the CF-XZ1200 in a patient with SAA.</p><p>Conception and design: Noriyuki Hirakawa, Katsuya Kitamura and Takao Itoi. Manuscript preparation: Noriyuki Hirakawa. Endoscopic procedures: Noriyuki Hirakawa and Katsuya Kitamura.</p>","PeriodicalId":16056,"journal":{"name":"Journal of Hepato‐Biliary‐Pancreatic Sciences","volume":"31 9","pages":"e53-e55"},"PeriodicalIF":3.2000,"publicationDate":"2024-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jhbp.12013","citationCount":"0","resultStr":"{\"title\":\"A case of complete removal of stacked common bile duct stones by peroral direct digital cholangioscopy in a patient with surgically altered anatomy\",\"authors\":\"Noriyuki Hirakawa, Katsuya Kitamura, Takao Itoi\",\"doi\":\"10.1002/jhbp.12013\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Treatment of common bile duct stones or anastomotic stenosis is challenging in patients with surgically altered anatomy (SAA). Although the clinical outcomes of balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography (BE-ERCP) have been improving in these patients,<span><sup>1-3</sup></span> stacked stones are still difficult to remove in some cases. There are also cases in which electrohydraulic lithotripsy (EHL) is required for the removal of stacked stones in patients with SAA.<span><sup>4</sup></span></p><p>The patient in this case was an 89-year-old man who had undergone Roux-en Y reconstruction after resection of gastric cancer. He was admitted to our hospital for treatment of cholangitis due to stacked common bile duct stones. BE-ERCP was attempted for bile duct drainage, but the papilla could not be identified and percutaneous transhepatic biliary drainage was performed. Then rendezvous BE-ERCP using the percutaneous transhepatic drainage route was performed (Figure 1). Although the papilla could be identified, the stacked stones were difficult to remove, and EHL was planned for the next session. Unfortunately, a peroral direct digital cholangioscope (SpyDS; Boston Scientific, Natick, Massachusetts, USA) with a caliber of 3.3 mm was not available for BE-ERCP because of the limited diameter of the accessory channel (3.2 mm). Therefore, ERCP was performed using a colonoscope (CF-XZ1200; Olympus Medical, Tokyo, Japan), in which the cholangioscope can be inserted via the accessory channel (3.7 mm).</p><p>The cholangioscope was inserted into the common bile duct via the CF-XZ1200 and showed that the common bile duct was filled with stacked stones. The stacked stones were crushed by EHL and cholangiography showed that the stones were reduced in size. The stones were completely removed using a mechanical lithotripter and basket catheter. The patient had a favorable course and was discharged (Figure 2).</p><p>This case demonstrates that stacked stones can be safely and effectively removed by EHL and other tools with the CF-XZ1200 in a patient with SAA.</p><p>Conception and design: Noriyuki Hirakawa, Katsuya Kitamura and Takao Itoi. Manuscript preparation: Noriyuki Hirakawa. Endoscopic procedures: Noriyuki Hirakawa and Katsuya Kitamura.</p>\",\"PeriodicalId\":16056,\"journal\":{\"name\":\"Journal of Hepato‐Biliary‐Pancreatic Sciences\",\"volume\":\"31 9\",\"pages\":\"e53-e55\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2024-06-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jhbp.12013\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Hepato‐Biliary‐Pancreatic Sciences\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jhbp.12013\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepato‐Biliary‐Pancreatic Sciences","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jhbp.12013","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
A case of complete removal of stacked common bile duct stones by peroral direct digital cholangioscopy in a patient with surgically altered anatomy
Treatment of common bile duct stones or anastomotic stenosis is challenging in patients with surgically altered anatomy (SAA). Although the clinical outcomes of balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography (BE-ERCP) have been improving in these patients,1-3 stacked stones are still difficult to remove in some cases. There are also cases in which electrohydraulic lithotripsy (EHL) is required for the removal of stacked stones in patients with SAA.4
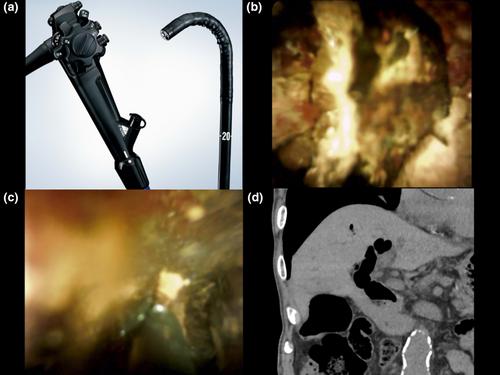
The patient in this case was an 89-year-old man who had undergone Roux-en Y reconstruction after resection of gastric cancer. He was admitted to our hospital for treatment of cholangitis due to stacked common bile duct stones. BE-ERCP was attempted for bile duct drainage, but the papilla could not be identified and percutaneous transhepatic biliary drainage was performed. Then rendezvous BE-ERCP using the percutaneous transhepatic drainage route was performed (Figure 1). Although the papilla could be identified, the stacked stones were difficult to remove, and EHL was planned for the next session. Unfortunately, a peroral direct digital cholangioscope (SpyDS; Boston Scientific, Natick, Massachusetts, USA) with a caliber of 3.3 mm was not available for BE-ERCP because of the limited diameter of the accessory channel (3.2 mm). Therefore, ERCP was performed using a colonoscope (CF-XZ1200; Olympus Medical, Tokyo, Japan), in which the cholangioscope can be inserted via the accessory channel (3.7 mm).
The cholangioscope was inserted into the common bile duct via the CF-XZ1200 and showed that the common bile duct was filled with stacked stones. The stacked stones were crushed by EHL and cholangiography showed that the stones were reduced in size. The stones were completely removed using a mechanical lithotripter and basket catheter. The patient had a favorable course and was discharged (Figure 2).
This case demonstrates that stacked stones can be safely and effectively removed by EHL and other tools with the CF-XZ1200 in a patient with SAA.
Conception and design: Noriyuki Hirakawa, Katsuya Kitamura and Takao Itoi. Manuscript preparation: Noriyuki Hirakawa. Endoscopic procedures: Noriyuki Hirakawa and Katsuya Kitamura.
期刊介绍:
The Journal of Hepato-Biliary-Pancreatic Sciences (JHBPS) is the leading peer-reviewed journal in the field of hepato-biliary-pancreatic sciences. JHBPS publishes articles dealing with clinical research as well as translational research on all aspects of this field. Coverage includes Original Article, Review Article, Images of Interest, Rapid Communication and an announcement section. Letters to the Editor and comments on the journal’s policies or content are also included. JHBPS welcomes submissions from surgeons, physicians, endoscopists, radiologists, oncologists, and pathologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


