{"title":"NT-proBNP水平过高和过低的心衰患者长期不良预后风险过高:一项为期 7 年的随访研究(NorthStar 试验)","authors":"","doi":"10.1016/j.ijcha.2024.101441","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>This study investigated excess risk in patients with heart failure with reduced left ventricular ejection fraction (HFrEF) with or without elevated levels of NT-proBNP (N-terminal pro-brain natriuretic peptide).</p></div><div><h3>Methods</h3><p>Patients with HFrEF from the NorthStar cohort (n = 1120) were matched on age, sex, and presence of AF (atrial fibrillation/flutter) to five controls without HFrEF from The Danish National Patient Registries. Patients were compared with controls before and after stratification according to baseline NT-proBNP levels, with cutoffs defined as </≥ 600 pg/ml in patients with sinus rhythm and </≥ 900 pg/ml in patients with AF. The primary composite endpoint was a 7-year risk of cardiovascular death or HF admission.</p></div><div><h3>Results</h3><p>In the HFrEF cohort, 704 patients had high NT-proBNP (median age, 73; mean left ventricular ejection fraction (LVEF), 33%). 416 patients had low NT-proBNP (median age, 65; LVEF, 30%). Patients from both groups were in NYHA class I-III. The primary endpoint occurred in 531 patients (75.4%) with HFrEF and elevated NT-proBNP, and 748 controls (21.3%) (risk difference, 54.2%; 95% confidence interval (CI) 50.7–57.6%). In comparison, it occurred in 199 patients (47.9%) with HFrEF and without elevated NT-proBNP, and 185 controls (8,9%) (risk difference, 38.9%; 95% CI 34.0–43.9%). Risk differences for all secondary endpoints were significant, except for overall mortality in the low NT-proBNP group (risk difference, 3.8%; 95% CI, −0.4–8.0%).</p></div><div><h3>Conclusion</h3><p>This study identified a significant excess risk in patients with HFrEF across various endpoints, which persisted after stratification into high and low levels of NT-proBNP.</p></div>","PeriodicalId":38026,"journal":{"name":"IJC Heart and Vasculature","volume":null,"pages":null},"PeriodicalIF":2.5000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2352906724001076/pdfft?md5=b29a5b5f0c4046e2c0d0d0097f1ff42c&pid=1-s2.0-S2352906724001076-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Excess long-term risk of adverse outcomes in heart failure patients with high and low levels of NT-proBNP: A 7-year follow-up study (NorthStar Trial)\",\"authors\":\"\",\"doi\":\"10.1016/j.ijcha.2024.101441\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>This study investigated excess risk in patients with heart failure with reduced left ventricular ejection fraction (HFrEF) with or without elevated levels of NT-proBNP (N-terminal pro-brain natriuretic peptide).</p></div><div><h3>Methods</h3><p>Patients with HFrEF from the NorthStar cohort (n = 1120) were matched on age, sex, and presence of AF (atrial fibrillation/flutter) to five controls without HFrEF from The Danish National Patient Registries. Patients were compared with controls before and after stratification according to baseline NT-proBNP levels, with cutoffs defined as </≥ 600 pg/ml in patients with sinus rhythm and </≥ 900 pg/ml in patients with AF. The primary composite endpoint was a 7-year risk of cardiovascular death or HF admission.</p></div><div><h3>Results</h3><p>In the HFrEF cohort, 704 patients had high NT-proBNP (median age, 73; mean left ventricular ejection fraction (LVEF), 33%). 416 patients had low NT-proBNP (median age, 65; LVEF, 30%). Patients from both groups were in NYHA class I-III. The primary endpoint occurred in 531 patients (75.4%) with HFrEF and elevated NT-proBNP, and 748 controls (21.3%) (risk difference, 54.2%; 95% confidence interval (CI) 50.7–57.6%). In comparison, it occurred in 199 patients (47.9%) with HFrEF and without elevated NT-proBNP, and 185 controls (8,9%) (risk difference, 38.9%; 95% CI 34.0–43.9%). Risk differences for all secondary endpoints were significant, except for overall mortality in the low NT-proBNP group (risk difference, 3.8%; 95% CI, −0.4–8.0%).</p></div><div><h3>Conclusion</h3><p>This study identified a significant excess risk in patients with HFrEF across various endpoints, which persisted after stratification into high and low levels of NT-proBNP.</p></div>\",\"PeriodicalId\":38026,\"journal\":{\"name\":\"IJC Heart and Vasculature\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2352906724001076/pdfft?md5=b29a5b5f0c4046e2c0d0d0097f1ff42c&pid=1-s2.0-S2352906724001076-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"IJC Heart and Vasculature\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2352906724001076\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"IJC Heart and Vasculature","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2352906724001076","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Excess long-term risk of adverse outcomes in heart failure patients with high and low levels of NT-proBNP: A 7-year follow-up study (NorthStar Trial)
Background
This study investigated excess risk in patients with heart failure with reduced left ventricular ejection fraction (HFrEF) with or without elevated levels of NT-proBNP (N-terminal pro-brain natriuretic peptide).
Methods
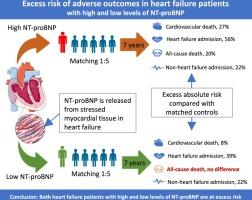
Patients with HFrEF from the NorthStar cohort (n = 1120) were matched on age, sex, and presence of AF (atrial fibrillation/flutter) to five controls without HFrEF from The Danish National Patient Registries. Patients were compared with controls before and after stratification according to baseline NT-proBNP levels, with cutoffs defined as </≥ 600 pg/ml in patients with sinus rhythm and </≥ 900 pg/ml in patients with AF. The primary composite endpoint was a 7-year risk of cardiovascular death or HF admission.
Results
In the HFrEF cohort, 704 patients had high NT-proBNP (median age, 73; mean left ventricular ejection fraction (LVEF), 33%). 416 patients had low NT-proBNP (median age, 65; LVEF, 30%). Patients from both groups were in NYHA class I-III. The primary endpoint occurred in 531 patients (75.4%) with HFrEF and elevated NT-proBNP, and 748 controls (21.3%) (risk difference, 54.2%; 95% confidence interval (CI) 50.7–57.6%). In comparison, it occurred in 199 patients (47.9%) with HFrEF and without elevated NT-proBNP, and 185 controls (8,9%) (risk difference, 38.9%; 95% CI 34.0–43.9%). Risk differences for all secondary endpoints were significant, except for overall mortality in the low NT-proBNP group (risk difference, 3.8%; 95% CI, −0.4–8.0%).
Conclusion
This study identified a significant excess risk in patients with HFrEF across various endpoints, which persisted after stratification into high and low levels of NT-proBNP.
期刊介绍:
IJC Heart & Vasculature is an online-only, open-access journal dedicated to publishing original articles and reviews (also Editorials and Letters to the Editor) which report on structural and functional cardiovascular pathology, with an emphasis on imaging and disease pathophysiology. Articles must be authentic, educational, clinically relevant, and original in their content and scientific approach. IJC Heart & Vasculature requires the highest standards of scientific integrity in order to promote reliable, reproducible and verifiable research findings. All authors are advised to consult the Principles of Ethical Publishing in the International Journal of Cardiology before submitting a manuscript. Submission of a manuscript to this journal gives the publisher the right to publish that paper if it is accepted. Manuscripts may be edited to improve clarity and expression.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


