{"title":"采用腹腔镜体腔内重叠吻合术(KYCC 2101)进行右侧结肠癌手术后吻合口漏的多中心前瞻性研究","authors":"Keisuke Kazama, Masakatsu Numata, Hiroyuki Mushiake, Nobuhiro Sugano, Teni Godai, Akio Higuchi, Tetsushi Ishiguro, Yosuke Atsumi, Satoru Shinoda, Aya Saito","doi":"10.1002/ags3.12831","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>Intracorporeal anastomosis (IA) is becoming increasingly popular and replacing extracorporeal anastomosis (EA) for reconstruction in laparoscopic and robotic surgery for right-sided colon cancer (LSRCC). Intracorporeal overlap anastomosis (IOA) is the most widely used IA technique. This study aimed to examine the safety of IOA by investigating its short-term results during the implementation phase.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This multicenter prospective cohort study was conducted by the Kanagawa Yokohama Colorectal Cancer (KYCC) Study Group. Patients with stage 1–3 colon cancer who planned to undergo LSRCC with IOA reconstruction were eligible. The incidence of anastomotic leakage (AL) of Clavien–Dindo (C–D) grade ≥3 was evaluated as the primary endpoint, and other surgical outcomes and postoperative complications of C–D grades ≥2 were the secondary endpoints.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 127 patients were enrolled, of whom 120 were finally analyzed. The incidence of C–D grade ≥2 complications was 8.3%. The incidence of C–D grade ≥3 AL was 0.8%. This trend was lower than that reported in previous randomized controlled trials (RCTs) and acceptable. Additionally, 1.7% of the patients developed abdominal abscesses, and no cases of anastomotic stenosis were observed. The median operative time was 257 min, and the reconstruction procedure required 32 min. Stapler closure of the enterotomy and facility experience of more than 30 cases were associated with a shorter reconstruction time during IOA.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>IOA is feasible and can be safely performed during the implementation phase in patients undergoing LSRCC.</p>\n </section>\n </div>","PeriodicalId":8030,"journal":{"name":"Annals of Gastroenterological Surgery","volume":"8 5","pages":"836-844"},"PeriodicalIF":2.9000,"publicationDate":"2024-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12831","citationCount":"0","resultStr":"{\"title\":\"Multicenter prospective study on anastomotic leakage after right-sided colon cancer surgery with laparoscopic intracorporeal overlap anastomosis (KYCC 2101)\",\"authors\":\"Keisuke Kazama, Masakatsu Numata, Hiroyuki Mushiake, Nobuhiro Sugano, Teni Godai, Akio Higuchi, Tetsushi Ishiguro, Yosuke Atsumi, Satoru Shinoda, Aya Saito\",\"doi\":\"10.1002/ags3.12831\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aim</h3>\\n \\n <p>Intracorporeal anastomosis (IA) is becoming increasingly popular and replacing extracorporeal anastomosis (EA) for reconstruction in laparoscopic and robotic surgery for right-sided colon cancer (LSRCC). Intracorporeal overlap anastomosis (IOA) is the most widely used IA technique. This study aimed to examine the safety of IOA by investigating its short-term results during the implementation phase.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This multicenter prospective cohort study was conducted by the Kanagawa Yokohama Colorectal Cancer (KYCC) Study Group. Patients with stage 1–3 colon cancer who planned to undergo LSRCC with IOA reconstruction were eligible. The incidence of anastomotic leakage (AL) of Clavien–Dindo (C–D) grade ≥3 was evaluated as the primary endpoint, and other surgical outcomes and postoperative complications of C–D grades ≥2 were the secondary endpoints.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 127 patients were enrolled, of whom 120 were finally analyzed. The incidence of C–D grade ≥2 complications was 8.3%. The incidence of C–D grade ≥3 AL was 0.8%. This trend was lower than that reported in previous randomized controlled trials (RCTs) and acceptable. Additionally, 1.7% of the patients developed abdominal abscesses, and no cases of anastomotic stenosis were observed. The median operative time was 257 min, and the reconstruction procedure required 32 min. Stapler closure of the enterotomy and facility experience of more than 30 cases were associated with a shorter reconstruction time during IOA.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>IOA is feasible and can be safely performed during the implementation phase in patients undergoing LSRCC.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8030,\"journal\":{\"name\":\"Annals of Gastroenterological Surgery\",\"volume\":\"8 5\",\"pages\":\"836-844\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-06-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12831\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterological Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12831\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterological Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12831","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
在腹腔镜和机器人手术治疗右侧结肠癌(LSRCC)时,体腔内吻合术(IA)正逐渐取代体外吻合术(EA)用于重建手术。体腔内重叠吻合术(IOA)是应用最广泛的IA技术。这项多中心前瞻性队列研究由神奈川横滨大肠癌(KYCC)研究小组进行。这项多中心前瞻性队列研究由神奈川横滨大肠癌研究小组(KYCC Study Group)开展。1-3期大肠癌患者计划接受IOA重建的LSRCC手术。以Clavien-Dindo(C-D)分级≥3级的吻合口漏(AL)发生率为主要终点,以C-D分级≥2级的其他手术结果和术后并发症为次要终点。C-D≥2级并发症的发生率为8.3%。C-D≥3级并发症的发生率为0.8%。这一趋势低于之前的随机对照试验(RCT),可以接受。此外,1.7%的患者出现腹腔脓肿,没有发现吻合口狭窄的病例。手术时间中位数为 257 分钟,重建过程需要 32 分钟。IOA是可行的,并且可以在LSRCC患者的实施阶段安全地进行。
Multicenter prospective study on anastomotic leakage after right-sided colon cancer surgery with laparoscopic intracorporeal overlap anastomosis (KYCC 2101)
Aim
Intracorporeal anastomosis (IA) is becoming increasingly popular and replacing extracorporeal anastomosis (EA) for reconstruction in laparoscopic and robotic surgery for right-sided colon cancer (LSRCC). Intracorporeal overlap anastomosis (IOA) is the most widely used IA technique. This study aimed to examine the safety of IOA by investigating its short-term results during the implementation phase.
Methods
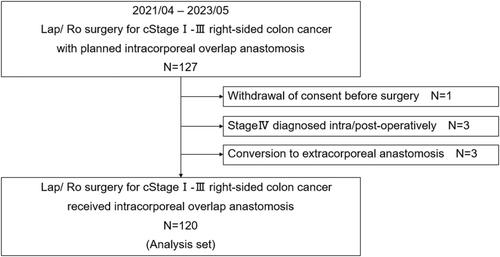
This multicenter prospective cohort study was conducted by the Kanagawa Yokohama Colorectal Cancer (KYCC) Study Group. Patients with stage 1–3 colon cancer who planned to undergo LSRCC with IOA reconstruction were eligible. The incidence of anastomotic leakage (AL) of Clavien–Dindo (C–D) grade ≥3 was evaluated as the primary endpoint, and other surgical outcomes and postoperative complications of C–D grades ≥2 were the secondary endpoints.
Results
A total of 127 patients were enrolled, of whom 120 were finally analyzed. The incidence of C–D grade ≥2 complications was 8.3%. The incidence of C–D grade ≥3 AL was 0.8%. This trend was lower than that reported in previous randomized controlled trials (RCTs) and acceptable. Additionally, 1.7% of the patients developed abdominal abscesses, and no cases of anastomotic stenosis were observed. The median operative time was 257 min, and the reconstruction procedure required 32 min. Stapler closure of the enterotomy and facility experience of more than 30 cases were associated with a shorter reconstruction time during IOA.
Conclusion
IOA is feasible and can be safely performed during the implementation phase in patients undergoing LSRCC.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


