Juan José Perales-Afán, Diego Aparicio-Pelaz, Sheila López-Triguero, Elena Llorente, Juan José Puente-Lanzarote, Marta Fabre
{"title":"25- 羟基维生素 D 的直接和间接参考区间:维生素 D 缺乏症并未真正流行。","authors":"Juan José Perales-Afán, Diego Aparicio-Pelaz, Sheila López-Triguero, Elena Llorente, Juan José Puente-Lanzarote, Marta Fabre","doi":"10.11613/BM.2024.020706","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Many studies report vitamin D (25-OH-D) deficiency, although there is no consensus among scientific societies on cut-offs and reference intervals (RI). The aim of this study is to establish and compare RI for serum 25-OH-D by direct and indirect methods.</p><p><strong>Materials and methods: </strong>Two studies were performed in Zaragoza (Spain). A retrospective study (N = 7222) between January 2017 and April 2019 was used for RI calculation by indirect method and a prospective study (N = 312) with healthy volunteers recruited in August 2019 and February 2020 for direct method. Seasonal differences were investigated. Measurements were performed on Cobas C8000 (Roche-Diagnostics, Basel, Switzerland) using electrochemiluminescence immunoassay technology.</p><p><strong>Results: </strong>Reference intervals (2.5-97.5 percentile and corresponding 95% confidence intervals, CIs) were as follows: by indirect method 5.6 ng/mL (5.4 to 5.8) - 57.2 ng/mL (55.2 to 59.8), in winter 5.4 ng/mL (5.2 to 5.7) - 55.7 ng/mL (53.6 to 58.4), while in summer 5.9 ng/mL (5.4 to 6.2) - 59.9 ng/mL (56.3 to 62.9). By direct method 9.0 ng/mL (5.7 to 9.5) - 41.4 ng/mL (37.6 to 48.0), in winter 7.4 ng/mL (3.9 to 8.6) - 34.6 ng/mL (30.6 to 51.5), while in summer 13.3 ng/mL (10.1 to 14.1) - 44.1 ng/mL (38.9 to 66.0). In both methods, RIs were higher in summer. A significant difference was observed in 25-OH-D median values between the two methods (P < 0.001).</p><p><strong>Conclusions: </strong>Reference interval calculation according to the studied area may be a useful tool to adapt the deficiency cut-offs for 25-OH-D. Our data support 25-OH-D values over 12.0 ng/mL for healthy population as sufficient, therefore current recommendations should be updated. In addition, differences in seasonality should be taken into account.</p>","PeriodicalId":94370,"journal":{"name":"Biochemia medica","volume":"34 2","pages":"020706"},"PeriodicalIF":1.8000,"publicationDate":"2024-06-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11177660/pdf/","citationCount":"0","resultStr":"{\"title\":\"Direct and indirect reference intervals of 25-hydroxyvitamin D: it is not a real vitamin D deficiency pandemic.\",\"authors\":\"Juan José Perales-Afán, Diego Aparicio-Pelaz, Sheila López-Triguero, Elena Llorente, Juan José Puente-Lanzarote, Marta Fabre\",\"doi\":\"10.11613/BM.2024.020706\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Many studies report vitamin D (25-OH-D) deficiency, although there is no consensus among scientific societies on cut-offs and reference intervals (RI). The aim of this study is to establish and compare RI for serum 25-OH-D by direct and indirect methods.</p><p><strong>Materials and methods: </strong>Two studies were performed in Zaragoza (Spain). A retrospective study (N = 7222) between January 2017 and April 2019 was used for RI calculation by indirect method and a prospective study (N = 312) with healthy volunteers recruited in August 2019 and February 2020 for direct method. Seasonal differences were investigated. Measurements were performed on Cobas C8000 (Roche-Diagnostics, Basel, Switzerland) using electrochemiluminescence immunoassay technology.</p><p><strong>Results: </strong>Reference intervals (2.5-97.5 percentile and corresponding 95% confidence intervals, CIs) were as follows: by indirect method 5.6 ng/mL (5.4 to 5.8) - 57.2 ng/mL (55.2 to 59.8), in winter 5.4 ng/mL (5.2 to 5.7) - 55.7 ng/mL (53.6 to 58.4), while in summer 5.9 ng/mL (5.4 to 6.2) - 59.9 ng/mL (56.3 to 62.9). By direct method 9.0 ng/mL (5.7 to 9.5) - 41.4 ng/mL (37.6 to 48.0), in winter 7.4 ng/mL (3.9 to 8.6) - 34.6 ng/mL (30.6 to 51.5), while in summer 13.3 ng/mL (10.1 to 14.1) - 44.1 ng/mL (38.9 to 66.0). In both methods, RIs were higher in summer. A significant difference was observed in 25-OH-D median values between the two methods (P < 0.001).</p><p><strong>Conclusions: </strong>Reference interval calculation according to the studied area may be a useful tool to adapt the deficiency cut-offs for 25-OH-D. Our data support 25-OH-D values over 12.0 ng/mL for healthy population as sufficient, therefore current recommendations should be updated. In addition, differences in seasonality should be taken into account.</p>\",\"PeriodicalId\":94370,\"journal\":{\"name\":\"Biochemia medica\",\"volume\":\"34 2\",\"pages\":\"020706\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-06-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11177660/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Biochemia medica\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.11613/BM.2024.020706\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biochemia medica","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.11613/BM.2024.020706","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Direct and indirect reference intervals of 25-hydroxyvitamin D: it is not a real vitamin D deficiency pandemic.
Introduction: Many studies report vitamin D (25-OH-D) deficiency, although there is no consensus among scientific societies on cut-offs and reference intervals (RI). The aim of this study is to establish and compare RI for serum 25-OH-D by direct and indirect methods.
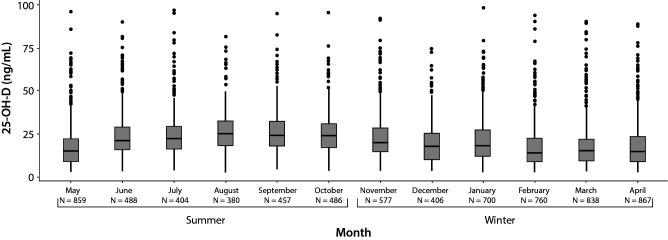
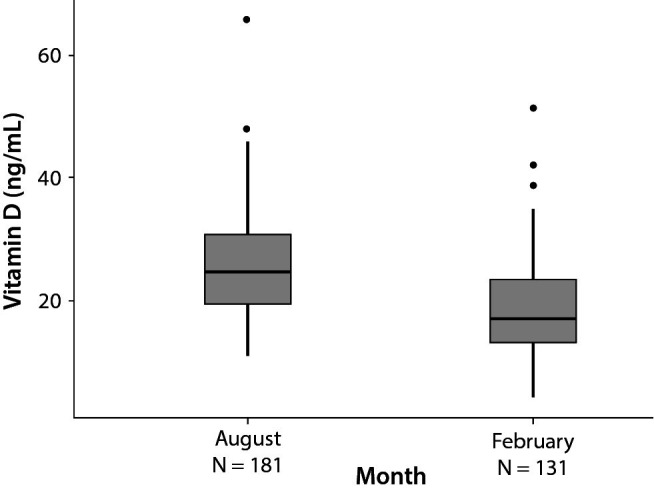
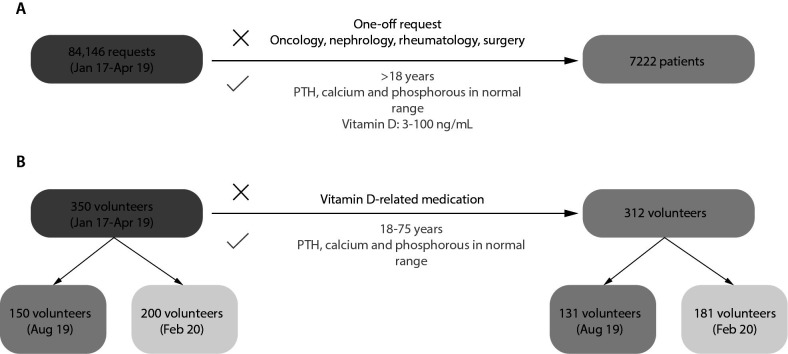
Materials and methods: Two studies were performed in Zaragoza (Spain). A retrospective study (N = 7222) between January 2017 and April 2019 was used for RI calculation by indirect method and a prospective study (N = 312) with healthy volunteers recruited in August 2019 and February 2020 for direct method. Seasonal differences were investigated. Measurements were performed on Cobas C8000 (Roche-Diagnostics, Basel, Switzerland) using electrochemiluminescence immunoassay technology.
Results: Reference intervals (2.5-97.5 percentile and corresponding 95% confidence intervals, CIs) were as follows: by indirect method 5.6 ng/mL (5.4 to 5.8) - 57.2 ng/mL (55.2 to 59.8), in winter 5.4 ng/mL (5.2 to 5.7) - 55.7 ng/mL (53.6 to 58.4), while in summer 5.9 ng/mL (5.4 to 6.2) - 59.9 ng/mL (56.3 to 62.9). By direct method 9.0 ng/mL (5.7 to 9.5) - 41.4 ng/mL (37.6 to 48.0), in winter 7.4 ng/mL (3.9 to 8.6) - 34.6 ng/mL (30.6 to 51.5), while in summer 13.3 ng/mL (10.1 to 14.1) - 44.1 ng/mL (38.9 to 66.0). In both methods, RIs were higher in summer. A significant difference was observed in 25-OH-D median values between the two methods (P < 0.001).
Conclusions: Reference interval calculation according to the studied area may be a useful tool to adapt the deficiency cut-offs for 25-OH-D. Our data support 25-OH-D values over 12.0 ng/mL for healthy population as sufficient, therefore current recommendations should be updated. In addition, differences in seasonality should be taken into account.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


