Anna E.C. Stoelinga , Maaike Biewenga , Joost P.H. Drenth , Xavier Verhelst , Adriaan J.P. van der Meer , Ynto S. de Boer , Gerd Bouma , Elsemieke S. de Vries , Robert C. Verdonk , Aad P. van der Berg , Johannes T. Brouwer , Thomas Vanwolleghem , Wim Lammers , Ulrich Beuers , Arantza Farina Sarasqueta , Joanne Verheij , Tania Roskams , Stijn Crobach , Maarten E. Tushuizen , Bart van Hoek , H.M. de Jonge
{"title":"联合疗法下 AIH-PBC 变异综合征的诊断标准和长期疗效","authors":"Anna E.C. Stoelinga , Maaike Biewenga , Joost P.H. Drenth , Xavier Verhelst , Adriaan J.P. van der Meer , Ynto S. de Boer , Gerd Bouma , Elsemieke S. de Vries , Robert C. Verdonk , Aad P. van der Berg , Johannes T. Brouwer , Thomas Vanwolleghem , Wim Lammers , Ulrich Beuers , Arantza Farina Sarasqueta , Joanne Verheij , Tania Roskams , Stijn Crobach , Maarten E. Tushuizen , Bart van Hoek , H.M. de Jonge","doi":"10.1016/j.jhepr.2024.101088","DOIUrl":null,"url":null,"abstract":"<div><h3>Background & Aims</h3><p>Autoimmune hepatitis (AIH) and primary biliary cholangitis (PBC) can co-exist in AIH-PBC, requiring combined treatment with immunosuppression and ursodeoxycholic acid (UDCA). The Paris criteria are commonly used to identify these patients; however, the optimal diagnostic criteria are unknown. We aimed to evaluate the use and clinical relevance of both Paris and Zhang criteria.</p></div><div><h3>Methods</h3><p>Eighty-three patients with a clinical suspicion of AIH-PBC who were treated with combination therapy were included. Histology was re-evaluated. Characteristics and long-term outcomes were retrospectively compared to patients with AIH and PBC.</p></div><div><h3>Results</h3><p>Seventeen (24%) patients treated with combination therapy fulfilled the Paris criteria. Fifty-two patients (70%) fulfilled the Zhang criteria. Patients who met Paris and Zhang criteria more often had inflammation and fibrosis on histology compared to patients only meeting the Zhang criteria. Ten-year liver transplant (LT)-free survival was 87.3% (95% CI 78.9–95.7%) in patients with AIH-PBC. This did not differ in patients in or outside the Paris or Zhang criteria (<em>p =</em> 0.46 and <em>p =</em> 0.40, respectively) or from AIH (<em>p =</em> 0.086). LT-free survival was significantly lower in patients with PBC and severe hepatic inflammation – not receiving immunosuppression – compared to those with AIH-PBC (65%; 95% CI 52.2–77.8% <em>vs</em>. 87%; 95% CI 83.2–90.8%; hazard ratio 0.52; <em>p =</em> 0.043).</p></div><div><h3>Conclusions</h3><p>In this study, patients with AIH-PBC outside Paris or Zhang criteria were frequently labeled as having AIH-PBC and were successfully treated with combination therapy with similar outcomes. LT-free survival was worse in patients with PBC and hepatic inflammation than in those treated as having AIH-PBC. More patients may benefit from combination therapy.</p></div><div><h3>Impact and implications</h3><p>This study demonstrated that patients with AIH-PBC variant syndrome treated with combined therapy consisting of immunosuppressants and ursodeoxycholic acid often do not fulfill the Paris criteria. They do however have comparable response to therapy and long-term outcomes as patients who do fulfill the diagnostic criteria. Additionally, patients with PBC and additional signs of hepatic inflammation have poorer long-term outcomes compared to patients treated as having AIH-PBC. These results implicate that a larger group of patients with features of both AIH and PBC may benefit from combined treatment. With our results, we call for improved consensus among experts in the field on the diagnosis and management of AIH-PBC variant syndrome.</p></div>","PeriodicalId":14764,"journal":{"name":"JHEP Reports","volume":"6 7","pages":"Article 101088"},"PeriodicalIF":9.5000,"publicationDate":"2024-06-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2589555924000922/pdfft?md5=a344652c95e7f2d2a73499cb23684adf&pid=1-s2.0-S2589555924000922-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Diagnostic criteria and long-term outcomes in AIH-PBC variant syndrome under combination therapy\",\"authors\":\"Anna E.C. Stoelinga , Maaike Biewenga , Joost P.H. Drenth , Xavier Verhelst , Adriaan J.P. van der Meer , Ynto S. de Boer , Gerd Bouma , Elsemieke S. de Vries , Robert C. Verdonk , Aad P. van der Berg , Johannes T. Brouwer , Thomas Vanwolleghem , Wim Lammers , Ulrich Beuers , Arantza Farina Sarasqueta , Joanne Verheij , Tania Roskams , Stijn Crobach , Maarten E. Tushuizen , Bart van Hoek , H.M. de Jonge\",\"doi\":\"10.1016/j.jhepr.2024.101088\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background & Aims</h3><p>Autoimmune hepatitis (AIH) and primary biliary cholangitis (PBC) can co-exist in AIH-PBC, requiring combined treatment with immunosuppression and ursodeoxycholic acid (UDCA). The Paris criteria are commonly used to identify these patients; however, the optimal diagnostic criteria are unknown. We aimed to evaluate the use and clinical relevance of both Paris and Zhang criteria.</p></div><div><h3>Methods</h3><p>Eighty-three patients with a clinical suspicion of AIH-PBC who were treated with combination therapy were included. Histology was re-evaluated. Characteristics and long-term outcomes were retrospectively compared to patients with AIH and PBC.</p></div><div><h3>Results</h3><p>Seventeen (24%) patients treated with combination therapy fulfilled the Paris criteria. Fifty-two patients (70%) fulfilled the Zhang criteria. Patients who met Paris and Zhang criteria more often had inflammation and fibrosis on histology compared to patients only meeting the Zhang criteria. Ten-year liver transplant (LT)-free survival was 87.3% (95% CI 78.9–95.7%) in patients with AIH-PBC. This did not differ in patients in or outside the Paris or Zhang criteria (<em>p =</em> 0.46 and <em>p =</em> 0.40, respectively) or from AIH (<em>p =</em> 0.086). LT-free survival was significantly lower in patients with PBC and severe hepatic inflammation – not receiving immunosuppression – compared to those with AIH-PBC (65%; 95% CI 52.2–77.8% <em>vs</em>. 87%; 95% CI 83.2–90.8%; hazard ratio 0.52; <em>p =</em> 0.043).</p></div><div><h3>Conclusions</h3><p>In this study, patients with AIH-PBC outside Paris or Zhang criteria were frequently labeled as having AIH-PBC and were successfully treated with combination therapy with similar outcomes. LT-free survival was worse in patients with PBC and hepatic inflammation than in those treated as having AIH-PBC. More patients may benefit from combination therapy.</p></div><div><h3>Impact and implications</h3><p>This study demonstrated that patients with AIH-PBC variant syndrome treated with combined therapy consisting of immunosuppressants and ursodeoxycholic acid often do not fulfill the Paris criteria. They do however have comparable response to therapy and long-term outcomes as patients who do fulfill the diagnostic criteria. Additionally, patients with PBC and additional signs of hepatic inflammation have poorer long-term outcomes compared to patients treated as having AIH-PBC. These results implicate that a larger group of patients with features of both AIH and PBC may benefit from combined treatment. With our results, we call for improved consensus among experts in the field on the diagnosis and management of AIH-PBC variant syndrome.</p></div>\",\"PeriodicalId\":14764,\"journal\":{\"name\":\"JHEP Reports\",\"volume\":\"6 7\",\"pages\":\"Article 101088\"},\"PeriodicalIF\":9.5000,\"publicationDate\":\"2024-06-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2589555924000922/pdfft?md5=a344652c95e7f2d2a73499cb23684adf&pid=1-s2.0-S2589555924000922-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JHEP Reports\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2589555924000922\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JHEP Reports","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2589555924000922","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景& 目的自身免疫性肝炎(AIH)和原发性胆汁性胆管炎(PBC)可在 AIH-PBC 中并存,需要联合使用免疫抑制剂和熊去氧胆酸(UDCA)进行治疗。巴黎标准通常用于识别这些患者,但最佳诊断标准尚不明确。我们旨在评估 Paris 标准和 Zhang 标准的使用情况和临床相关性。重新评估组织学。结果17例(24%)接受联合治疗的患者符合巴黎标准,52例患者(70%)符合张标准。52名患者(70%)符合张氏标准。与仅符合张氏标准的患者相比,符合巴黎和张氏标准的患者在组织学上更常出现炎症和纤维化。AIH-PBC患者的十年无肝移植存活率为87.3%(95% CI为78.9-95.7%)。这在符合或不符合巴黎标准或张氏标准(分别为 p = 0.46 和 p = 0.40)或 AIH(p = 0.086)的患者中没有差异。结论在这项研究中,未达到巴黎标准或张氏标准的AIH-PBC患者经常被标记为AIH-PBC,并成功接受了联合治疗,结果相似。PBC和肝脏炎症患者的无LT生存率比AIH-PBC患者更差。影响和意义这项研究表明,接受由免疫抑制剂和熊去氧胆酸组成的联合疗法治疗的AIH-PBC变异综合征患者往往不符合巴黎标准。不过,他们对治疗的反应和长期疗效与符合诊断标准的患者相当。此外,与接受 AIH-PBC 治疗的患者相比,有 PBC 和其他肝脏炎症体征的患者的长期疗效较差。这些结果表明,更多同时具有 AIH 和 PBC 特征的患者可能会从联合治疗中获益。根据我们的研究结果,我们呼吁该领域的专家就 AIH-PBC 变异综合征的诊断和管理达成更多共识。
Diagnostic criteria and long-term outcomes in AIH-PBC variant syndrome under combination therapy
Background & Aims
Autoimmune hepatitis (AIH) and primary biliary cholangitis (PBC) can co-exist in AIH-PBC, requiring combined treatment with immunosuppression and ursodeoxycholic acid (UDCA). The Paris criteria are commonly used to identify these patients; however, the optimal diagnostic criteria are unknown. We aimed to evaluate the use and clinical relevance of both Paris and Zhang criteria.
Methods
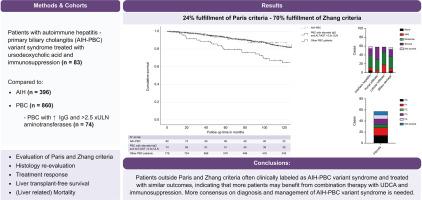
Eighty-three patients with a clinical suspicion of AIH-PBC who were treated with combination therapy were included. Histology was re-evaluated. Characteristics and long-term outcomes were retrospectively compared to patients with AIH and PBC.
Results
Seventeen (24%) patients treated with combination therapy fulfilled the Paris criteria. Fifty-two patients (70%) fulfilled the Zhang criteria. Patients who met Paris and Zhang criteria more often had inflammation and fibrosis on histology compared to patients only meeting the Zhang criteria. Ten-year liver transplant (LT)-free survival was 87.3% (95% CI 78.9–95.7%) in patients with AIH-PBC. This did not differ in patients in or outside the Paris or Zhang criteria (p = 0.46 and p = 0.40, respectively) or from AIH (p = 0.086). LT-free survival was significantly lower in patients with PBC and severe hepatic inflammation – not receiving immunosuppression – compared to those with AIH-PBC (65%; 95% CI 52.2–77.8% vs. 87%; 95% CI 83.2–90.8%; hazard ratio 0.52; p = 0.043).
Conclusions
In this study, patients with AIH-PBC outside Paris or Zhang criteria were frequently labeled as having AIH-PBC and were successfully treated with combination therapy with similar outcomes. LT-free survival was worse in patients with PBC and hepatic inflammation than in those treated as having AIH-PBC. More patients may benefit from combination therapy.
Impact and implications
This study demonstrated that patients with AIH-PBC variant syndrome treated with combined therapy consisting of immunosuppressants and ursodeoxycholic acid often do not fulfill the Paris criteria. They do however have comparable response to therapy and long-term outcomes as patients who do fulfill the diagnostic criteria. Additionally, patients with PBC and additional signs of hepatic inflammation have poorer long-term outcomes compared to patients treated as having AIH-PBC. These results implicate that a larger group of patients with features of both AIH and PBC may benefit from combined treatment. With our results, we call for improved consensus among experts in the field on the diagnosis and management of AIH-PBC variant syndrome.
期刊介绍:
JHEP Reports is an open access journal that is affiliated with the European Association for the Study of the Liver (EASL). It serves as a companion journal to the highly respected Journal of Hepatology.
The primary objective of JHEP Reports is to publish original papers and reviews that contribute to the advancement of knowledge in the field of liver diseases. The journal covers a wide range of topics, including basic, translational, and clinical research. It also focuses on global issues in hepatology, with particular emphasis on areas such as clinical trials, novel diagnostics, precision medicine and therapeutics, cancer research, cellular and molecular studies, artificial intelligence, microbiome research, epidemiology, and cutting-edge technologies.
In summary, JHEP Reports is dedicated to promoting scientific discoveries and innovations in liver diseases through the publication of high-quality research papers and reviews covering various aspects of hepatology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


