室内空气质量二氧化碳指南:综述。
IF 4.7
3区 医学
Q2 ENVIRONMENTAL SCIENCES
Journal of Exposure Science and Environmental Epidemiology
Pub Date : 2024-06-13
DOI:10.1038/s41370-024-00694-7
引用次数: 0
摘要
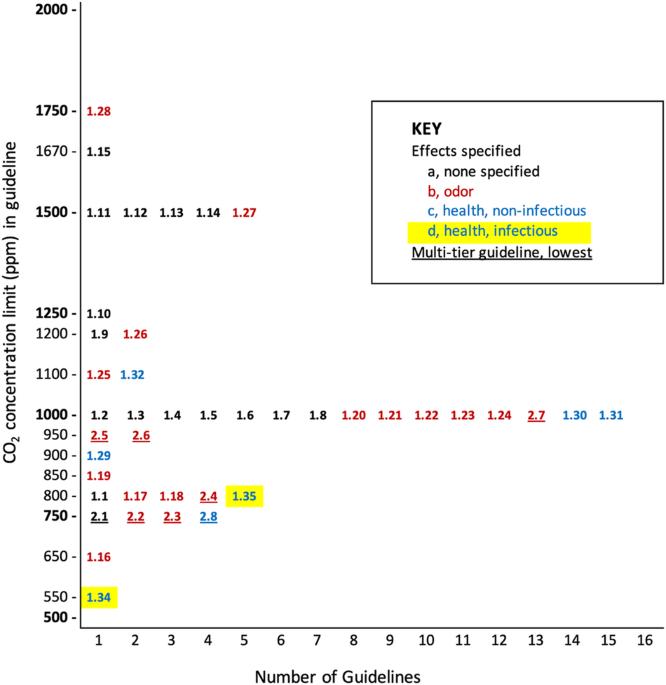
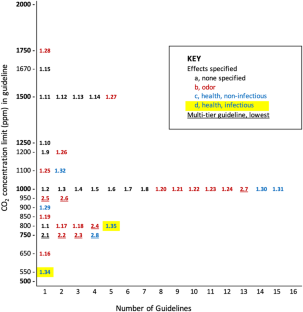
背景:自 COVID-19 大流行以来,建筑通风对保护健康的重要性得到了更广泛的认可。建筑物内的室外空气流通可以稀释室内产生的空气污染物(包括生物气溶胶),并减少居住者接触污染物的机会。许多国家和组织都制定了最低通风率(VRs)的建议指南或强制标准,以保持室内空气质量(IAQ)。由于直接测量通风率通常比较困难,因此许多室内空气质量指南都规定了二氧化碳(CO2)的室内浓度限值,将建筑物内居住者呼出的二氧化碳作为通风率的指标。虽然室内二氧化碳指南很常见,但各种二氧化碳限值的证据基础并不明确:回顾全球现行的室内 CO2 指南以及所提供的支持性证据:方法:我们确定了世界范围内基于 CO2 的室内空气质量或通风指南,以及所提供的支持性证据。我们排除了二氧化碳水平≥5000 ppm的职业指南:在已确定的 43 份指南中,35 份设定了单一的二氧化碳浓度限值,8 份设定了多层限值;16 份未提及需要控制的具体人体影响,19 份仅规定了气味不满,5 份规定了非传染性健康影响,3 份规定了空气传播传染病。最常见的室内二氧化碳限值为 1000 ppm。有 13 份指南规定二氧化碳的最大限值为扩展的时间加权平均值,但没有一份指南提供证据证明平均限值与对居住者的影响有关。在仅有的 18 份引用证据支持限值设定的指南中,我们发现有 8 份指南的证据具有说服力。在这 8 份指南中,有 7 份指南设定了控制气味感知的限值。其中一份指南针对具体的空间用途和占用情况,提供了 17 个有科学依据的二氧化碳限值,以控制 COVID-19 在室内的远距离传播:影响:许多现行的室内二氧化碳(CO2)室内空气质量指南都没有规定要控制的不良影响。最常提到的影响是对气味的不满,很少有人提到健康,有三项提到了对传染病的控制。只有一项二氧化碳指南是根据控制 COVID-19 在空气中传播的科学模型制定的。大多数指南都没有为指定的限制提供支持性证据;很少有指南提供有说服力的证据。对于为所有建筑物的室内空气质量设定一个二氧化碳限值、将室内空气质量的二氧化碳限值设定为延长时间加权平均值或使用一次性二氧化碳测量来验证所需的 VR,没有明显的科学依据。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Carbon dioxide guidelines for indoor air quality: a review
The importance of building ventilation to protect health has been more widely recognized since the COVID-19 pandemic. Outdoor air ventilation in buildings dilutes indoor-generated air pollutants (including bioaerosols) and reduces resulting occupant exposures. Many countries and organizations have advisory guidelines or mandatory standards for minimum ventilation rates (VRs) to maintain indoor air quality (IAQ). Because directly measuring VRs is often difficult, many IAQ guidelines instead specify indoor concentration limits for carbon dioxide (CO2), using CO2 exhaled by building occupants as an indicator of VR. Although indoor CO2 guidelines are common, the evidence basis for the various CO2 limits has not been clear. To review current indoor CO2 guidelines worldwide and the supportive evidence provided. We identified worldwide CO2-based guidelines for IAQ or ventilation, along with any supportive evidence provided. We excluded occupational guidelines for CO2 levels ≥5000 ppm. Among 43 guidelines identified, 35 set single CO2 concentration limits and eight set multi-tiered limits; 16 mentioned no specific human effect to be controlled, 19 specified only odor dissatisfaction, five specified non-infectious health effects, and three specified airborne infectious disease transmission. The most common indoor CO2 limit was 1000 ppm. Thirteen guidelines specified maximum CO2 limits as extended time-weighted averages, none with evidence linking averaged limits to occupant effects. Of only 18 guidelines citing evidence to support limits set, we found this evidence persuasive for eight. Among these eight guidelines, seven set limits to control odor perception. One provided 17 scientifically-based CO2 limits, for specific example space uses and occupancies, to control long-range COVID-19 transmission indoors. Many current indoor carbon dioxide (CO2) guidelines for indoor air quality specified no adverse effects intended for control. Odor dissatisfaction was the effect mentioned most frequently, few mentioned health, and three mentioned control of infectious disease. Only one CO2 guideline was developed from scientific models to control airborne transmission of COVID‐19. Most guidelines provided no supportive evidence for specified limits; few provided persuasive evidence. No scientific basis is apparent for setting one CO2 limit for IAQ across all buildings, setting a CO2 limit for IAQ as an extended time-weighted average, or using any arbitrary one-time CO2 measurement to verify a desired VR.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

CiteScore
8.90
自引率
6.70%
发文量
93
审稿时长
3 months
期刊介绍:
Journal of Exposure Science and Environmental Epidemiology (JESEE) aims to be the premier and authoritative source of information on advances in exposure science for professionals in a wide range of environmental and public health disciplines.
JESEE publishes original peer-reviewed research presenting significant advances in exposure science and exposure analysis, including development and application of the latest technologies for measuring exposures, and innovative computational approaches for translating novel data streams to characterize and predict exposures. The types of papers published in the research section of JESEE are original research articles, translation studies, and correspondence. Reported results should further understanding of the relationship between environmental exposure and human health, describe evaluated novel exposure science tools, or demonstrate potential of exposure science to enable decisions and actions that promote and protect human health.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


