Nicole Cyrille-Superville MD, Sriram D. Rao MBBS, Jason P. Feliberti MD, Priyesh A. Patel MD, Kamala Swayampakala PhD, Shashank S. Sinha MD, MSc, Eric I. Jeng MD, Rohan M. Goswami MD, David F. Snipelisky MD, Aubrie M. Carroll MD, Samer S. Najjar MD, Mark Belkin MD, Jonathan Grinstein MD, FACC, the FLIGHT Working Group
{"title":"PREDICT HF:利用新型血液动力学参数对晚期心力衰竭进行风险分层","authors":"Nicole Cyrille-Superville MD, Sriram D. Rao MBBS, Jason P. Feliberti MD, Priyesh A. Patel MD, Kamala Swayampakala PhD, Shashank S. Sinha MD, MSc, Eric I. Jeng MD, Rohan M. Goswami MD, David F. Snipelisky MD, Aubrie M. Carroll MD, Samer S. Najjar MD, Mark Belkin MD, Jonathan Grinstein MD, FACC, the FLIGHT Working Group","doi":"10.1002/clc.24277","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Invasive hemodynamics are fundamental in assessing patients with advanced heart failure (HF). Several novel hemodynamic parameters have been studied; however, the relative prognostic potential remains ill-defined.</p>\n </section>\n \n <section>\n \n <h3> Hypothesis</h3>\n \n <p>Advanced hemodynamic parameters provide additional prognostication beyond the standard hemodynamic assessment.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Patients from the PRognostic Evaluation During Invasive CaTheterization for Heart Failure (PREDICT-HF) registry who underwent right heart catheterization (RHC) were included in the analysis. The primary endpoint was survival to orthotopic heart transplant (OHT) or durable left ventricular assist device (LVAD), or death within 6 months of RHC.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Of 846 patients included, 176 (21%) met the primary endpoint. In a multivariate model that included traditional hemodynamic variables, pulmonary capillary wedge pressure (PCWP) (OR: 1.10, 1.04−1.15, <i>p</i> < .001), and cardiac index (CI) (OR: 0.86, 0.81−0.92, <i>p</i> < .001) were shown to be predictive of adverse outcomes. In a separate multivariate model that incorporated advanced hemodynamic parameters, cardiac power output (CPO) (OR: 0.76, 0.71−0.83, <i>p</i> < .001), aortic pulsatility index (API) (OR: 0.94, 0.91−0.96, <i>p</i> < .001), and pulmonary artery pulsatility index (OR: 1.02, 1.00−1.03, <i>p</i> .027) were all significantly associated with the primary outcome. Positively concordant API and CPO afforded the best freedom from the endpoint (94.7%), whilst negatively concordant API and CPO had the worst freedom from the endpoint (61.5%, <i>p</i> < .001). Those with discordant API and CPO had similar freedom from the endpoint.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>The advanced hemodynamic parameters API and CPO are independently associated with death or the need for OHT or LVAD within 6 months. Further prospective studies are needed to validate these parameters and elucidate their role in patients with advanced HF.</p>\n </section>\n </div>","PeriodicalId":2,"journal":{"name":"ACS Applied Bio Materials","volume":null,"pages":null},"PeriodicalIF":4.6000,"publicationDate":"2024-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24277","citationCount":"0","resultStr":"{\"title\":\"PREDICT HF: Risk stratification in advanced heart failure using novel hemodynamic parameters\",\"authors\":\"Nicole Cyrille-Superville MD, Sriram D. Rao MBBS, Jason P. Feliberti MD, Priyesh A. Patel MD, Kamala Swayampakala PhD, Shashank S. Sinha MD, MSc, Eric I. Jeng MD, Rohan M. Goswami MD, David F. Snipelisky MD, Aubrie M. Carroll MD, Samer S. Najjar MD, Mark Belkin MD, Jonathan Grinstein MD, FACC, the FLIGHT Working Group\",\"doi\":\"10.1002/clc.24277\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Invasive hemodynamics are fundamental in assessing patients with advanced heart failure (HF). Several novel hemodynamic parameters have been studied; however, the relative prognostic potential remains ill-defined.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Hypothesis</h3>\\n \\n <p>Advanced hemodynamic parameters provide additional prognostication beyond the standard hemodynamic assessment.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Patients from the PRognostic Evaluation During Invasive CaTheterization for Heart Failure (PREDICT-HF) registry who underwent right heart catheterization (RHC) were included in the analysis. The primary endpoint was survival to orthotopic heart transplant (OHT) or durable left ventricular assist device (LVAD), or death within 6 months of RHC.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Of 846 patients included, 176 (21%) met the primary endpoint. In a multivariate model that included traditional hemodynamic variables, pulmonary capillary wedge pressure (PCWP) (OR: 1.10, 1.04−1.15, <i>p</i> < .001), and cardiac index (CI) (OR: 0.86, 0.81−0.92, <i>p</i> < .001) were shown to be predictive of adverse outcomes. In a separate multivariate model that incorporated advanced hemodynamic parameters, cardiac power output (CPO) (OR: 0.76, 0.71−0.83, <i>p</i> < .001), aortic pulsatility index (API) (OR: 0.94, 0.91−0.96, <i>p</i> < .001), and pulmonary artery pulsatility index (OR: 1.02, 1.00−1.03, <i>p</i> .027) were all significantly associated with the primary outcome. Positively concordant API and CPO afforded the best freedom from the endpoint (94.7%), whilst negatively concordant API and CPO had the worst freedom from the endpoint (61.5%, <i>p</i> < .001). Those with discordant API and CPO had similar freedom from the endpoint.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>The advanced hemodynamic parameters API and CPO are independently associated with death or the need for OHT or LVAD within 6 months. Further prospective studies are needed to validate these parameters and elucidate their role in patients with advanced HF.</p>\\n </section>\\n </div>\",\"PeriodicalId\":2,\"journal\":{\"name\":\"ACS Applied Bio Materials\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2024-06-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24277\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACS Applied Bio Materials\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clc.24277\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MATERIALS SCIENCE, BIOMATERIALS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Bio Materials","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.24277","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MATERIALS SCIENCE, BIOMATERIALS","Score":null,"Total":0}
PREDICT HF: Risk stratification in advanced heart failure using novel hemodynamic parameters
Background
Invasive hemodynamics are fundamental in assessing patients with advanced heart failure (HF). Several novel hemodynamic parameters have been studied; however, the relative prognostic potential remains ill-defined.
Hypothesis
Advanced hemodynamic parameters provide additional prognostication beyond the standard hemodynamic assessment.
Methods
Patients from the PRognostic Evaluation During Invasive CaTheterization for Heart Failure (PREDICT-HF) registry who underwent right heart catheterization (RHC) were included in the analysis. The primary endpoint was survival to orthotopic heart transplant (OHT) or durable left ventricular assist device (LVAD), or death within 6 months of RHC.
Results
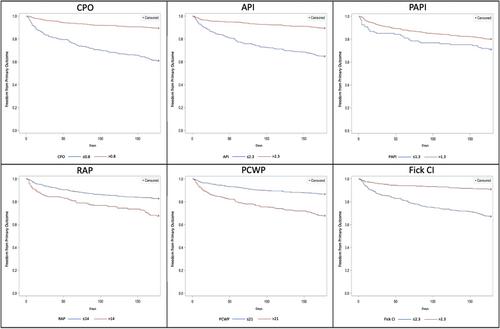
Of 846 patients included, 176 (21%) met the primary endpoint. In a multivariate model that included traditional hemodynamic variables, pulmonary capillary wedge pressure (PCWP) (OR: 1.10, 1.04−1.15, p < .001), and cardiac index (CI) (OR: 0.86, 0.81−0.92, p < .001) were shown to be predictive of adverse outcomes. In a separate multivariate model that incorporated advanced hemodynamic parameters, cardiac power output (CPO) (OR: 0.76, 0.71−0.83, p < .001), aortic pulsatility index (API) (OR: 0.94, 0.91−0.96, p < .001), and pulmonary artery pulsatility index (OR: 1.02, 1.00−1.03, p .027) were all significantly associated with the primary outcome. Positively concordant API and CPO afforded the best freedom from the endpoint (94.7%), whilst negatively concordant API and CPO had the worst freedom from the endpoint (61.5%, p < .001). Those with discordant API and CPO had similar freedom from the endpoint.
Conclusion
The advanced hemodynamic parameters API and CPO are independently associated with death or the need for OHT or LVAD within 6 months. Further prospective studies are needed to validate these parameters and elucidate their role in patients with advanced HF.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


