Nicholas Mai, Sara Myers, Sherry Shen, Stephanie Downs-Canner, Mark Robson, Larry Norton, Yuan Chen, Tiffany Traina, Nour Abuhadra
{"title":"在治疗三阴性乳腺癌的 KEYNOTE522 改良方案中采用剂量密集的多柔比星加环磷酰胺。","authors":"Nicholas Mai, Sara Myers, Sherry Shen, Stephanie Downs-Canner, Mark Robson, Larry Norton, Yuan Chen, Tiffany Traina, Nour Abuhadra","doi":"10.1038/s41523-024-00643-5","DOIUrl":null,"url":null,"abstract":"<p><p>The KEYNOTE-522 (KN522) regimen for neoadjuvant treatment of triple negative breast cancer (TNBC) utilized q3week dosing for doxorubicin plus cyclophosphamide (AC); however, dose-dense AC (ddAC) has demonstrated superior overall survival (OS) compared to q3week AC in anthracycline and taxane-based regimens. We performed a retrospective analysis assessing the use of ddAC in KN522 and the impact of sequencing ddAC before or after carboplatin/paclitaxel (CbT) plus pembrolizumab on multiple outcomes. 128 patients with TNBC were included. Overall pathologic complete response (pCR) rate of 56%. Sequencing of ddAC vs CbT first showed no difference in pCR rate (ddAC 55% vs. CbT 58%, p = 0.77). However, ddAC first compared to CbT first correlated with a significant increase in the incidence of overall treatment delays (ddAC 70% vs. CbT 51%, p = 0.03), with cytopenias most frequent (ddAC 59% vs. CbT 31%, p = 0.001). ddAC in a modified KN522 regimen is safe, tolerable, and effective. Efficacy is comparable regardless of chemotherapy sequencing, but ddAC first is significantly associated with higher rates of treatment delays and cytopenias.</p>","PeriodicalId":19247,"journal":{"name":"NPJ Breast Cancer","volume":"10 1","pages":"39"},"PeriodicalIF":6.5000,"publicationDate":"2024-06-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11150442/pdf/","citationCount":"0","resultStr":"{\"title\":\"Dose dense doxorubicin plus cyclophosphamide in a modified KEYNOTE522 regimen for triple negative breast cancer.\",\"authors\":\"Nicholas Mai, Sara Myers, Sherry Shen, Stephanie Downs-Canner, Mark Robson, Larry Norton, Yuan Chen, Tiffany Traina, Nour Abuhadra\",\"doi\":\"10.1038/s41523-024-00643-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The KEYNOTE-522 (KN522) regimen for neoadjuvant treatment of triple negative breast cancer (TNBC) utilized q3week dosing for doxorubicin plus cyclophosphamide (AC); however, dose-dense AC (ddAC) has demonstrated superior overall survival (OS) compared to q3week AC in anthracycline and taxane-based regimens. We performed a retrospective analysis assessing the use of ddAC in KN522 and the impact of sequencing ddAC before or after carboplatin/paclitaxel (CbT) plus pembrolizumab on multiple outcomes. 128 patients with TNBC were included. Overall pathologic complete response (pCR) rate of 56%. Sequencing of ddAC vs CbT first showed no difference in pCR rate (ddAC 55% vs. CbT 58%, p = 0.77). However, ddAC first compared to CbT first correlated with a significant increase in the incidence of overall treatment delays (ddAC 70% vs. CbT 51%, p = 0.03), with cytopenias most frequent (ddAC 59% vs. CbT 31%, p = 0.001). ddAC in a modified KN522 regimen is safe, tolerable, and effective. Efficacy is comparable regardless of chemotherapy sequencing, but ddAC first is significantly associated with higher rates of treatment delays and cytopenias.</p>\",\"PeriodicalId\":19247,\"journal\":{\"name\":\"NPJ Breast Cancer\",\"volume\":\"10 1\",\"pages\":\"39\"},\"PeriodicalIF\":6.5000,\"publicationDate\":\"2024-06-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11150442/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NPJ Breast Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41523-024-00643-5\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NPJ Breast Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41523-024-00643-5","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
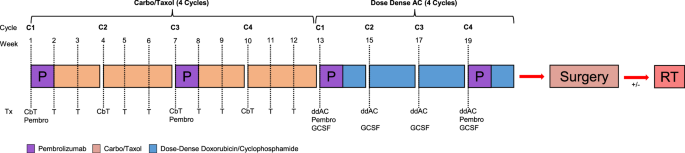
Dose dense doxorubicin plus cyclophosphamide in a modified KEYNOTE522 regimen for triple negative breast cancer.
The KEYNOTE-522 (KN522) regimen for neoadjuvant treatment of triple negative breast cancer (TNBC) utilized q3week dosing for doxorubicin plus cyclophosphamide (AC); however, dose-dense AC (ddAC) has demonstrated superior overall survival (OS) compared to q3week AC in anthracycline and taxane-based regimens. We performed a retrospective analysis assessing the use of ddAC in KN522 and the impact of sequencing ddAC before or after carboplatin/paclitaxel (CbT) plus pembrolizumab on multiple outcomes. 128 patients with TNBC were included. Overall pathologic complete response (pCR) rate of 56%. Sequencing of ddAC vs CbT first showed no difference in pCR rate (ddAC 55% vs. CbT 58%, p = 0.77). However, ddAC first compared to CbT first correlated with a significant increase in the incidence of overall treatment delays (ddAC 70% vs. CbT 51%, p = 0.03), with cytopenias most frequent (ddAC 59% vs. CbT 31%, p = 0.001). ddAC in a modified KN522 regimen is safe, tolerable, and effective. Efficacy is comparable regardless of chemotherapy sequencing, but ddAC first is significantly associated with higher rates of treatment delays and cytopenias.
期刊介绍:
npj Breast Cancer publishes original research articles, reviews, brief correspondence, meeting reports, editorial summaries and hypothesis generating observations which could be unexplained or preliminary findings from experiments, novel ideas, or the framing of new questions that need to be solved. Featured topics of the journal include imaging, immunotherapy, molecular classification of disease, mechanism-based therapies largely targeting signal transduction pathways, carcinogenesis including hereditary susceptibility and molecular epidemiology, survivorship issues including long-term toxicities of treatment and secondary neoplasm occurrence, the biophysics of cancer, mechanisms of metastasis and their perturbation, and studies of the tumor microenvironment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


