Aurora J Grutman, Kelli Gilliam, Ankith P Maremanda, Corey Able, Una Choi, Mark N Alshak, Taylor P Kohn
{"title":"按急性和长期 COVID、住院状态和使用血管加压药分层比较 SARS 冠状病毒 2 感染后勃起功能障碍的风险:美国大型索赔数据库分析。","authors":"Aurora J Grutman, Kelli Gilliam, Ankith P Maremanda, Corey Able, Una Choi, Mark N Alshak, Taylor P Kohn","doi":"10.1038/s41443-024-00913-7","DOIUrl":null,"url":null,"abstract":"<p><p>No study has yet assessed the risk of developing erectile dysfunction (ED) after a diagnosis of long COVID, defined by the Centers for Disease Control and Prevention as the persistence or presence of new symptoms at least 4 weeks after initial SARS-CoV-2 infection, when compared to those diagnosed with acute COVID or cases in which more severe treatment is required. To assess these risks, we queried the TriNetX COVID-19 Research Network from December 1st 2020 through June 2023. Men aged ≥ 18 diagnosed with long COVID were compared to those diagnosed with acute COVID and analyses were performed to compare men who were/were not hospitalized within 1 month of acute COVID diagnosis and men who did/did not need vasopressors. Cohorts were propensity score matched and compared for differences in new ED diagnosis and/or prescription of phosphodiesterase-5 inhibitors (PDE5i). After propensity score matching, the long and acute COVID cohorts included 2839 men with an average age of 54.5±16.7 and 55.1±17.1 years respectively (p = 0.21). Men with long COVID were more likely to develop ED or be prescribed PDE5i (3.63%) when compared to men with only acute COVID infections (2.61%) [RR 1.39; 95% CI 1.04, 1.87]. There was no statistically significant risk of developing ED or being prescribed PDE5i for individuals who received vasopressors [RR 0.92; 95% CI 0.77,1.10] or were hospitalized [RR 0.93; 95% CI 0.82,1.06].</p>","PeriodicalId":14068,"journal":{"name":"International Journal of Impotence Research","volume":" ","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2024-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Comparing risk of post infection erectile dysfunction following SARS Coronavirus 2 stratified by acute and long COVID, hospitalization status, and vasopressor administration: a U.S. large claims database analysis.\",\"authors\":\"Aurora J Grutman, Kelli Gilliam, Ankith P Maremanda, Corey Able, Una Choi, Mark N Alshak, Taylor P Kohn\",\"doi\":\"10.1038/s41443-024-00913-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>No study has yet assessed the risk of developing erectile dysfunction (ED) after a diagnosis of long COVID, defined by the Centers for Disease Control and Prevention as the persistence or presence of new symptoms at least 4 weeks after initial SARS-CoV-2 infection, when compared to those diagnosed with acute COVID or cases in which more severe treatment is required. To assess these risks, we queried the TriNetX COVID-19 Research Network from December 1st 2020 through June 2023. Men aged ≥ 18 diagnosed with long COVID were compared to those diagnosed with acute COVID and analyses were performed to compare men who were/were not hospitalized within 1 month of acute COVID diagnosis and men who did/did not need vasopressors. Cohorts were propensity score matched and compared for differences in new ED diagnosis and/or prescription of phosphodiesterase-5 inhibitors (PDE5i). After propensity score matching, the long and acute COVID cohorts included 2839 men with an average age of 54.5±16.7 and 55.1±17.1 years respectively (p = 0.21). Men with long COVID were more likely to develop ED or be prescribed PDE5i (3.63%) when compared to men with only acute COVID infections (2.61%) [RR 1.39; 95% CI 1.04, 1.87]. There was no statistically significant risk of developing ED or being prescribed PDE5i for individuals who received vasopressors [RR 0.92; 95% CI 0.77,1.10] or were hospitalized [RR 0.93; 95% CI 0.82,1.06].</p>\",\"PeriodicalId\":14068,\"journal\":{\"name\":\"International Journal of Impotence Research\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-05-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Impotence Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41443-024-00913-7\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Impotence Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41443-024-00913-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
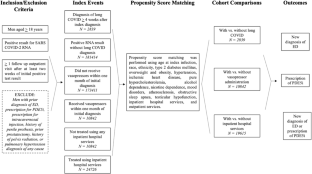
美国疾病控制和预防中心(Centers for Disease Control and Prevention)将长COVID定义为初次感染SARS-CoV-2病毒至少4周后症状持续存在或出现新症状,目前还没有研究评估与诊断为急性COVID或需要更严重治疗的病例相比,诊断为长COVID后出现勃起功能障碍(ED)的风险。为了评估这些风险,我们从 2020 年 12 月 1 日至 2023 年 6 月对 TriNetX COVID-19 研究网络进行了查询。将确诊为长期 COVID 的≥18 岁男性与确诊为急性 COVID 的男性进行了比较,并对确诊为急性 COVID 后 1 个月内住院/未住院的男性和需要/不需要血管加压的男性进行了分析比较。对各组进行倾向评分匹配,并比较新诊断出ED和/或开具磷酸二酯酶-5抑制剂(PDE5i)处方的差异。经过倾向得分匹配后,长期和急性COVID队列包括2839名男性,平均年龄分别为54.5±16.7岁和55.1±17.1岁(p = 0.21)。与仅感染急性 COVID 的男性(2.61%)相比,感染长期 COVID 的男性更有可能出现 ED 或被处方 PDE5i(3.63%)[RR 1.39; 95% CI 1.04, 1.87]。接受血管加压剂[RR 0.92; 95% CI 0.77,1.10]或住院治疗[RR 0.93; 95% CI 0.82,1.06]的患者发生ED或被处方PDE5i的风险在统计学上并不显著。
Comparing risk of post infection erectile dysfunction following SARS Coronavirus 2 stratified by acute and long COVID, hospitalization status, and vasopressor administration: a U.S. large claims database analysis.
No study has yet assessed the risk of developing erectile dysfunction (ED) after a diagnosis of long COVID, defined by the Centers for Disease Control and Prevention as the persistence or presence of new symptoms at least 4 weeks after initial SARS-CoV-2 infection, when compared to those diagnosed with acute COVID or cases in which more severe treatment is required. To assess these risks, we queried the TriNetX COVID-19 Research Network from December 1st 2020 through June 2023. Men aged ≥ 18 diagnosed with long COVID were compared to those diagnosed with acute COVID and analyses were performed to compare men who were/were not hospitalized within 1 month of acute COVID diagnosis and men who did/did not need vasopressors. Cohorts were propensity score matched and compared for differences in new ED diagnosis and/or prescription of phosphodiesterase-5 inhibitors (PDE5i). After propensity score matching, the long and acute COVID cohorts included 2839 men with an average age of 54.5±16.7 and 55.1±17.1 years respectively (p = 0.21). Men with long COVID were more likely to develop ED or be prescribed PDE5i (3.63%) when compared to men with only acute COVID infections (2.61%) [RR 1.39; 95% CI 1.04, 1.87]. There was no statistically significant risk of developing ED or being prescribed PDE5i for individuals who received vasopressors [RR 0.92; 95% CI 0.77,1.10] or were hospitalized [RR 0.93; 95% CI 0.82,1.06].
期刊介绍:
International Journal of Impotence Research: The Journal of Sexual Medicine addresses sexual medicine for both genders as an interdisciplinary field. This includes basic science researchers, urologists, endocrinologists, cardiologists, family practitioners, gynecologists, internists, neurologists, psychiatrists, psychologists, radiologists and other health care clinicians.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


