Felicity L Brown, Frederik Steen, Karine Taha, Gabriela V Koppenol-Gonzalez, May Aoun, Richard Bryant, Mark J D Jordans
{"title":"为生活在黎巴嫩弱势社区的青少年验证阿拉伯语版本的儿童心理社会困扰筛选器和儿科症状清单。","authors":"Felicity L Brown, Frederik Steen, Karine Taha, Gabriela V Koppenol-Gonzalez, May Aoun, Richard Bryant, Mark J D Jordans","doi":"10.1186/s13033-024-00640-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In humanitarian settings, brief screening instruments for child psychological distress have potential to assist in assessing prevalence, monitoring outcomes, and identifying children and adolescents in most need of scarce resources, given few mental health professionals for diagnostic services. Yet, there are few validated screening tools available, particularly in Arabic.</p><p><strong>Methods: </strong>We translated and adapted the Child Psychosocial Distress Screener (CPDS) and the Pediatric Symptom Checklist (PSC) and conducted a validation study with 85 adolescents (aged 10-15) in Lebanon. We assessed internal consistency; test-retest reliability; convergent validity between adolescent- and caregiver-report and between the two measures; ability to distinguish between clinical and non-clinical samples; and concurrent validity against psychiatrist interview using the Kiddie Schedule for Affective Disorders and Schizophrenia.</p><p><strong>Results: </strong>The translated and adapted child-reported PSC-17 and PSC-35, and caregiver-reported PSC-35 all showed adequate internal consistency and test-retest reliability and high concurrent validity with psychiatrist interview and were able to distinguish between clinical and non-clinical samples. However, the caregiver-reported PSC-17 did not demonstrate adequate performance in this setting. Child-reported versions of the PSC outperformed caregiver-reported versions and the 35-item PSC scales showed stronger performance than 17-item scales. The CPDS showed adequate convergent validity with the PSC, ability to distinguish between clinical and non-clinical samples, and concurrent validity with psychiatrist interview. Internal consistency was low for the CPDS, likely due to the nature of the brief risk-screening tool. There were discrepancies between caregiver and child-reports, worthy of future investigation. For indication of any diagnosis requiring treatment, we recommend cut-offs of 5 for CPDS, 12 for child-reported PSC-17, 21 for child-reported PSC-35, and 26 for caregiver-reported PSC-35.</p><p><strong>Conclusions: </strong>The Arabic PSC and CPDS are reliable and valid instruments for use as primary screening tools in Lebanon. Further research is needed to understand discrepancies between adolescent and caregiver reports, and optimal methods of using multiple informants.</p>","PeriodicalId":47752,"journal":{"name":"International Journal of Mental Health Systems","volume":"18 1","pages":"21"},"PeriodicalIF":3.8000,"publicationDate":"2024-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11137983/pdf/","citationCount":"0","resultStr":"{\"title\":\"Validation of Arabic versions of the child psychosocial distress screener and pediatric symptom checklist for young adolescents living in vulnerable communities in Lebanon.\",\"authors\":\"Felicity L Brown, Frederik Steen, Karine Taha, Gabriela V Koppenol-Gonzalez, May Aoun, Richard Bryant, Mark J D Jordans\",\"doi\":\"10.1186/s13033-024-00640-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In humanitarian settings, brief screening instruments for child psychological distress have potential to assist in assessing prevalence, monitoring outcomes, and identifying children and adolescents in most need of scarce resources, given few mental health professionals for diagnostic services. Yet, there are few validated screening tools available, particularly in Arabic.</p><p><strong>Methods: </strong>We translated and adapted the Child Psychosocial Distress Screener (CPDS) and the Pediatric Symptom Checklist (PSC) and conducted a validation study with 85 adolescents (aged 10-15) in Lebanon. We assessed internal consistency; test-retest reliability; convergent validity between adolescent- and caregiver-report and between the two measures; ability to distinguish between clinical and non-clinical samples; and concurrent validity against psychiatrist interview using the Kiddie Schedule for Affective Disorders and Schizophrenia.</p><p><strong>Results: </strong>The translated and adapted child-reported PSC-17 and PSC-35, and caregiver-reported PSC-35 all showed adequate internal consistency and test-retest reliability and high concurrent validity with psychiatrist interview and were able to distinguish between clinical and non-clinical samples. However, the caregiver-reported PSC-17 did not demonstrate adequate performance in this setting. Child-reported versions of the PSC outperformed caregiver-reported versions and the 35-item PSC scales showed stronger performance than 17-item scales. The CPDS showed adequate convergent validity with the PSC, ability to distinguish between clinical and non-clinical samples, and concurrent validity with psychiatrist interview. Internal consistency was low for the CPDS, likely due to the nature of the brief risk-screening tool. There were discrepancies between caregiver and child-reports, worthy of future investigation. For indication of any diagnosis requiring treatment, we recommend cut-offs of 5 for CPDS, 12 for child-reported PSC-17, 21 for child-reported PSC-35, and 26 for caregiver-reported PSC-35.</p><p><strong>Conclusions: </strong>The Arabic PSC and CPDS are reliable and valid instruments for use as primary screening tools in Lebanon. Further research is needed to understand discrepancies between adolescent and caregiver reports, and optimal methods of using multiple informants.</p>\",\"PeriodicalId\":47752,\"journal\":{\"name\":\"International Journal of Mental Health Systems\",\"volume\":\"18 1\",\"pages\":\"21\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2024-05-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11137983/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Mental Health Systems\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13033-024-00640-y\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PSYCHIATRY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Mental Health Systems","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13033-024-00640-y","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PSYCHIATRY","Score":null,"Total":0}
Validation of Arabic versions of the child psychosocial distress screener and pediatric symptom checklist for young adolescents living in vulnerable communities in Lebanon.
Background: In humanitarian settings, brief screening instruments for child psychological distress have potential to assist in assessing prevalence, monitoring outcomes, and identifying children and adolescents in most need of scarce resources, given few mental health professionals for diagnostic services. Yet, there are few validated screening tools available, particularly in Arabic.
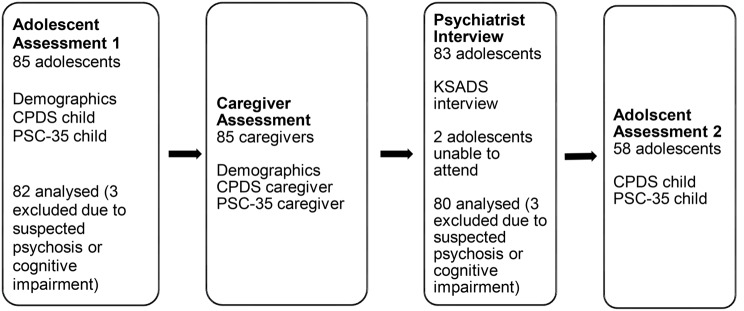
Methods: We translated and adapted the Child Psychosocial Distress Screener (CPDS) and the Pediatric Symptom Checklist (PSC) and conducted a validation study with 85 adolescents (aged 10-15) in Lebanon. We assessed internal consistency; test-retest reliability; convergent validity between adolescent- and caregiver-report and between the two measures; ability to distinguish between clinical and non-clinical samples; and concurrent validity against psychiatrist interview using the Kiddie Schedule for Affective Disorders and Schizophrenia.
Results: The translated and adapted child-reported PSC-17 and PSC-35, and caregiver-reported PSC-35 all showed adequate internal consistency and test-retest reliability and high concurrent validity with psychiatrist interview and were able to distinguish between clinical and non-clinical samples. However, the caregiver-reported PSC-17 did not demonstrate adequate performance in this setting. Child-reported versions of the PSC outperformed caregiver-reported versions and the 35-item PSC scales showed stronger performance than 17-item scales. The CPDS showed adequate convergent validity with the PSC, ability to distinguish between clinical and non-clinical samples, and concurrent validity with psychiatrist interview. Internal consistency was low for the CPDS, likely due to the nature of the brief risk-screening tool. There were discrepancies between caregiver and child-reports, worthy of future investigation. For indication of any diagnosis requiring treatment, we recommend cut-offs of 5 for CPDS, 12 for child-reported PSC-17, 21 for child-reported PSC-35, and 26 for caregiver-reported PSC-35.
Conclusions: The Arabic PSC and CPDS are reliable and valid instruments for use as primary screening tools in Lebanon. Further research is needed to understand discrepancies between adolescent and caregiver reports, and optimal methods of using multiple informants.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


