{"title":"接受经导管主动脉瓣置换术的出院患者在术后 30 天内出现的高分级主动脉瓣阻滞","authors":"","doi":"10.1016/j.shj.2024.100317","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Conduction disease is an important and common complication post-transcatheter aortic valve replacement (TAVR). Previously, we developed a conduction disease risk stratification and management protocol post-TAVR. This study aims to evaluate high-grade aortic valve block (HAVB) incidence and risk factors in a large cohort undergoing ambulatory cardiac monitoring post-TAVR according to conduction risk grouping.</p></div><div><h3>Methods</h3><p>This single-center, retrospective study evaluated all patients discharged on ambulatory cardiac monitoring between 2016 and 2021 and stratified them into 3 groups based on electrocardiogram predictors of HAVB risk (group 1 [low], group 2 [intermediate], and group 3 [high]). HAVB was defined as ≥2 consecutive nonconducted P waves in sinus rhythm or bradycardia <50 beats/minute with a fixed rate for atrial fibrillation/flutter. Descriptive statistics were used to show the incidence and timeline, while logistic regression was utilized to evaluate predictors of HAVB.</p></div><div><h3>Results</h3><p>Five hundred twenty-eight patients were included (median age 80 years [74-85]; 43.8% female). Forty-one patients (7.8%) developed HAVB during ambulatory monitoring (68% were asymptomatic). Over a median follow-up of 2 years (1.3-2.7), the overall mortality rate was 15.0% (30-day mortality rate of 0.57%, n = 3). Risk factors for HAVB were male sex (odds ratio [OR] = 2.46, <em>p</em> = 0.02, 95% CI = 1.21-5.43), baseline right bundle branch block (OR = 2.80, <em>p</em> = 0.01, 95% CI = 1.17-6.19), and post-TAVR QRS >150 ms (OR = 2.16, <em>p</em> = 0.03, 95% CI = 1.01-4.40). The negative predictive value for patients in groups 1 and 2 for 30-day HAVB was 95.0 and 93.8%, respectively.</p></div><div><h3>Conclusions</h3><p>The risk of 30-day HAVB post-TAVR on ambulatory monitoring post-TAVR varies according to post-TAVR electrocardiogram findings, and a 3-group algorithm effectively identifies groups with a low negative predictive value for HAVB.</p></div>","PeriodicalId":36053,"journal":{"name":"Structural Heart","volume":"8 4","pages":"Article 100317"},"PeriodicalIF":1.4000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2474870624000654/pdfft?md5=a068e70f14d7024f3f3d40417d2d999f&pid=1-s2.0-S2474870624000654-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Thirty-Day High-Grade Aortic Valve Block Post-Transcatheter Aortic Valve Replacement in Patients Discharged on Heart Rhythm Monitor\",\"authors\":\"\",\"doi\":\"10.1016/j.shj.2024.100317\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Conduction disease is an important and common complication post-transcatheter aortic valve replacement (TAVR). Previously, we developed a conduction disease risk stratification and management protocol post-TAVR. This study aims to evaluate high-grade aortic valve block (HAVB) incidence and risk factors in a large cohort undergoing ambulatory cardiac monitoring post-TAVR according to conduction risk grouping.</p></div><div><h3>Methods</h3><p>This single-center, retrospective study evaluated all patients discharged on ambulatory cardiac monitoring between 2016 and 2021 and stratified them into 3 groups based on electrocardiogram predictors of HAVB risk (group 1 [low], group 2 [intermediate], and group 3 [high]). HAVB was defined as ≥2 consecutive nonconducted P waves in sinus rhythm or bradycardia <50 beats/minute with a fixed rate for atrial fibrillation/flutter. Descriptive statistics were used to show the incidence and timeline, while logistic regression was utilized to evaluate predictors of HAVB.</p></div><div><h3>Results</h3><p>Five hundred twenty-eight patients were included (median age 80 years [74-85]; 43.8% female). Forty-one patients (7.8%) developed HAVB during ambulatory monitoring (68% were asymptomatic). Over a median follow-up of 2 years (1.3-2.7), the overall mortality rate was 15.0% (30-day mortality rate of 0.57%, n = 3). Risk factors for HAVB were male sex (odds ratio [OR] = 2.46, <em>p</em> = 0.02, 95% CI = 1.21-5.43), baseline right bundle branch block (OR = 2.80, <em>p</em> = 0.01, 95% CI = 1.17-6.19), and post-TAVR QRS >150 ms (OR = 2.16, <em>p</em> = 0.03, 95% CI = 1.01-4.40). The negative predictive value for patients in groups 1 and 2 for 30-day HAVB was 95.0 and 93.8%, respectively.</p></div><div><h3>Conclusions</h3><p>The risk of 30-day HAVB post-TAVR on ambulatory monitoring post-TAVR varies according to post-TAVR electrocardiogram findings, and a 3-group algorithm effectively identifies groups with a low negative predictive value for HAVB.</p></div>\",\"PeriodicalId\":36053,\"journal\":{\"name\":\"Structural Heart\",\"volume\":\"8 4\",\"pages\":\"Article 100317\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2474870624000654/pdfft?md5=a068e70f14d7024f3f3d40417d2d999f&pid=1-s2.0-S2474870624000654-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Structural Heart\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2474870624000654\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Structural Heart","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2474870624000654","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Thirty-Day High-Grade Aortic Valve Block Post-Transcatheter Aortic Valve Replacement in Patients Discharged on Heart Rhythm Monitor
Background
Conduction disease is an important and common complication post-transcatheter aortic valve replacement (TAVR). Previously, we developed a conduction disease risk stratification and management protocol post-TAVR. This study aims to evaluate high-grade aortic valve block (HAVB) incidence and risk factors in a large cohort undergoing ambulatory cardiac monitoring post-TAVR according to conduction risk grouping.
Methods
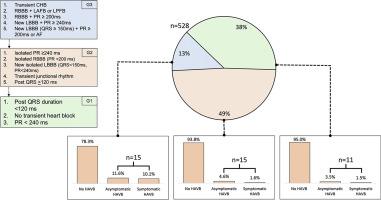
This single-center, retrospective study evaluated all patients discharged on ambulatory cardiac monitoring between 2016 and 2021 and stratified them into 3 groups based on electrocardiogram predictors of HAVB risk (group 1 [low], group 2 [intermediate], and group 3 [high]). HAVB was defined as ≥2 consecutive nonconducted P waves in sinus rhythm or bradycardia <50 beats/minute with a fixed rate for atrial fibrillation/flutter. Descriptive statistics were used to show the incidence and timeline, while logistic regression was utilized to evaluate predictors of HAVB.
Results
Five hundred twenty-eight patients were included (median age 80 years [74-85]; 43.8% female). Forty-one patients (7.8%) developed HAVB during ambulatory monitoring (68% were asymptomatic). Over a median follow-up of 2 years (1.3-2.7), the overall mortality rate was 15.0% (30-day mortality rate of 0.57%, n = 3). Risk factors for HAVB were male sex (odds ratio [OR] = 2.46, p = 0.02, 95% CI = 1.21-5.43), baseline right bundle branch block (OR = 2.80, p = 0.01, 95% CI = 1.17-6.19), and post-TAVR QRS >150 ms (OR = 2.16, p = 0.03, 95% CI = 1.01-4.40). The negative predictive value for patients in groups 1 and 2 for 30-day HAVB was 95.0 and 93.8%, respectively.
Conclusions
The risk of 30-day HAVB post-TAVR on ambulatory monitoring post-TAVR varies according to post-TAVR electrocardiogram findings, and a 3-group algorithm effectively identifies groups with a low negative predictive value for HAVB.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


