Gin S. Malhi, Uyen Le, Cornelia Kaufmann, Erica Bell
{"title":"在拉莫三嗪中加入艾司卡胺治疗重度抑郁症:组合协同作用、增强作用,还是两者皆无?","authors":"Gin S. Malhi, Uyen Le, Cornelia Kaufmann, Erica Bell","doi":"10.1111/bdi.13448","DOIUrl":null,"url":null,"abstract":"<p>In an investigator-initiated study<sup>1</sup> designed to determine the positioning of esketamine in the treatment (PoET) of depression, we have treated patients with severe depression. As it is a naturalistic study, we have no stipulations as to the antidepressant treatment the person is taking when commencing add-on esketamine therapy, which is administered via bi-weekly insufflation under medical supervision. Most patients that are referred are taking SSRIs, SNRIs or TCAs, and occasionally are taking MAOIs or novel agents such as vortioxetine. However, in one patient who had trialled most treatments, the physician had resorted to trialling lamotrigine even though the patient had no history of bipolar disorder, possibly because of the complexity of the illness (number of comorbidities) and lack of response.</p><p>It is this case, of a 44-year-old Caucasian female (LE) with a current psychiatric history of treatment resistant depression (TRD), along with generalized anxiety disorder (GAD), obsessive-compulsive disorder (OCD) and iatrogenic benzodiazepine dependence that we present here. Previous diagnoses also included orthorexia in recovery and substance misuse in young adulthood. Her medical history includes osteoporosis and ulcerative colitis, but she has been off steroids since 2015, and does not smoke, consume alcohol or use substances.</p><p>In late 2018, LE, then 40 years old, was diagnosed with major depressive disorder with anxiety. There was no significant precipitant for her depressive episodes and because of her illness, she stopped working in 2019. Her depressive symptoms included sadness, numbness, anhedonia, low self-worth, feelings of helplessness and hopelessness, loss of appetite, detachment and passive suicidal ideation. She described her depression as “<i>depression with unbearable pain</i>”, and she was “<i>unable to see the future</i>”. In addition to receiving psychological and dietetic treatments weekly, she also trialled multiple pharmacological treatments including SSRIs, SNRIs, TCAs, MAOIs, atypical antipsychotics and lithium augmentation (see Figure 1). She experienced a partial response with some medications but also had severe side effects. She also underwent a course of rTMS, which she reported “<i>did nothing for me, I felt like it did less than an SSRI</i>”.</p><p>In January 2024, the patient was referred to the CADE clinic<sup>2</sup> and screened for PoET. After an extensive assessment process, we deemed the patient suitable for enrolment. She consented and commenced the study in January 2024. As per our protocol, she received esketamine treatments twice weekly for 4 weeks. At the time of enrolment, LE was taking lamotrigine 200 mg daily, diazepam 4.5 mg daily (slowly weaning off, but kept at a stable dose for the duration of the trial) and suvorexant for sleep. She completed a baseline questionnaire and received her first esketamine treatment in January 2024. She completed the course by mid-February having received eight esketamine treatments in total. She completed weekly questionnaires that included standard depression symptom scales, as well as daily questionnaires comprising bespoke items throughout the duration of the study. Completion of the daily questionnaires was actively monitored to ensure accurate data collection. In addition, a comprehensive post-treatment questionnaire containing the same scales used in the baseline questionnaire, was completed after 4 weeks of esketamine treatment.</p><p>The use of esketamine is relatively new and it is being trialled alongside well-established antidepressant treatments in the management of depression.<span><sup>1</sup></span> The PoET study aims to characterise the clinical profile of patients in which esketamine would be best suited, and in those that benefit, determine which antidepressants are most likely to respond to esketamine enhancement.</p><p>During esketamine treatments, LE experienced side effects such as mild dissociation and transient increased blood pressure, both of which were to be expected and resolved 1 hour after treatment administration. After week 1 of esketamine (56 mg), she reported “<i>feeling better and sleeping better</i>” (Quick Inventory of Depressive Symptoms—Clinician rated [QIDS-C] = 21). After Week 2 of esketamine (84 mg), she reported an uplift in mood immediately post treatment that was sustained for 24 h, but the effect did not remain beyond this day (QIDS-C = 14). After Week 3 of esketamine (84 mg), LE reported an uplift in her mood post treatments, and her passive suicidal ideation had completely stopped (QIDS-C = 10). After Week 4 of esketamine (84 mg), she reported a “<i>definite uplift in mood and felt hungry for the first time in a long time</i>” along with a “<i>noticeable drop in anxiety</i>”. She also noted that the effect of esketamine seems to have been sustained and she described this as “<i>[my] mood continues to remain stable and energy level is good and [I am] able to carry out necessary task[s]</i>”. LE also reported that she “<i>seem[s] to be thinking clearer and enjoy[s] some activities without thinking everything in life is a chore</i>” (QIDS-C = 6).</p><p>As per protocol, LE attended a follow-up assessment 3 weeks after the last esketamine treatment and appeared to be smiling more. She reported that she was feeling better, with a noticeable increase in motivation and capacity for exercise, and her passive suicidal ideation remained absent. She also noted that she was coping better with ongoing psychosocial stressors. While she did notice a slight drop in motivation since the last treatment, her motivation remained heightened overall as compared to baseline. Both LE's partner and her children noted her improvement, commenting that she is less tearful and is going out more. LE continues to see a psychologist and dietician regularly.</p><p>Prior to esketamine treatments, LE scored 32 on the Montgomery-Asberg Depression Rating Scale (MADRS), 17 on the Hamilton Depression rating scale (HAM-D), and 4 on the Clinical Global Impressions Scale (CGI). After 4 weeks of esketamine treatment, she scored 8, 7 and 11 on these three scales, respectively (improvements of 24, 6 and 7 points on each scale).</p><p>Figure 2 shows that overall, there was notable improvement in energy and emotion and that even with respect to cognitive functioning there was a trend towards improvement, which was modest because of a high starting point at baseline. Importantly, there is a clear decrease in anhedonia, anxiety, irritability and LE reported a sudden cessation of her passive suicidal ideation (pink shading) from day 13 onwards. Significantly, this remained absent for the remainder of the trial and 3 weeks after study completion at a follow-up assessment.</p><p>Poor or incomplete response to antidepressants is common and novel treatments and strategies are urgently needed. One approach that is widely utilised but under investigated is that of combinations of medications. Combinations of treatments are seldom studied because they do not readily lend themselves to the randomised-controlled trial (RCT) paradigm. Therefore, naturalistic studies are needed to identify those patients that respond to medications when prescribed in combination with other agents, as is often the case in real-world practice.</p><p>In this case study, we have identified some benefits from adding esketamine to lamotrigine and speculate that this may reflect either synergism or augmentation, although given it is a single case study, it has to be borne in mind that it might be neither.</p><p>The PoET study and U.L.'s position is funded by an investigator-initiated grant from Janssen-Cilag, however the authors received no funding for the writing of this article.</p><p>The authors G.S.M., U.L. and E.B. are co-investigators in the PoET Study, Clinical Trial Number: ACTRN12623001068651. G.S.M. has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier; and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. He is the recipient of an investigator-initiated grant from Janssen-Cilag (PoET Study), joint grant funding from the University of Sydney and National Taiwan University (Ignition Grant) and grant funding from The North Foundation. E.B. has received joint grant funding from the University of Sydney and National Taiwan University (Ignition Grant) and grant funding from The North Foundation. U.L. is employed through funding from an investigator-initiated grant from Janssen-Cilag for the PoET Study. C.K. referred the patient (LE) to the PoET Study.</p>","PeriodicalId":8959,"journal":{"name":"Bipolar Disorders","volume":"26 5","pages":"500-504"},"PeriodicalIF":4.5000,"publicationDate":"2024-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bdi.13448","citationCount":"0","resultStr":"{\"title\":\"Adding esketamine to lamotrigine to treat major depression: Combinatorial synergism, augmentation, or neither?\",\"authors\":\"Gin S. Malhi, Uyen Le, Cornelia Kaufmann, Erica Bell\",\"doi\":\"10.1111/bdi.13448\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>In an investigator-initiated study<sup>1</sup> designed to determine the positioning of esketamine in the treatment (PoET) of depression, we have treated patients with severe depression. As it is a naturalistic study, we have no stipulations as to the antidepressant treatment the person is taking when commencing add-on esketamine therapy, which is administered via bi-weekly insufflation under medical supervision. Most patients that are referred are taking SSRIs, SNRIs or TCAs, and occasionally are taking MAOIs or novel agents such as vortioxetine. However, in one patient who had trialled most treatments, the physician had resorted to trialling lamotrigine even though the patient had no history of bipolar disorder, possibly because of the complexity of the illness (number of comorbidities) and lack of response.</p><p>It is this case, of a 44-year-old Caucasian female (LE) with a current psychiatric history of treatment resistant depression (TRD), along with generalized anxiety disorder (GAD), obsessive-compulsive disorder (OCD) and iatrogenic benzodiazepine dependence that we present here. Previous diagnoses also included orthorexia in recovery and substance misuse in young adulthood. Her medical history includes osteoporosis and ulcerative colitis, but she has been off steroids since 2015, and does not smoke, consume alcohol or use substances.</p><p>In late 2018, LE, then 40 years old, was diagnosed with major depressive disorder with anxiety. There was no significant precipitant for her depressive episodes and because of her illness, she stopped working in 2019. Her depressive symptoms included sadness, numbness, anhedonia, low self-worth, feelings of helplessness and hopelessness, loss of appetite, detachment and passive suicidal ideation. She described her depression as “<i>depression with unbearable pain</i>”, and she was “<i>unable to see the future</i>”. In addition to receiving psychological and dietetic treatments weekly, she also trialled multiple pharmacological treatments including SSRIs, SNRIs, TCAs, MAOIs, atypical antipsychotics and lithium augmentation (see Figure 1). She experienced a partial response with some medications but also had severe side effects. She also underwent a course of rTMS, which she reported “<i>did nothing for me, I felt like it did less than an SSRI</i>”.</p><p>In January 2024, the patient was referred to the CADE clinic<sup>2</sup> and screened for PoET. After an extensive assessment process, we deemed the patient suitable for enrolment. She consented and commenced the study in January 2024. As per our protocol, she received esketamine treatments twice weekly for 4 weeks. At the time of enrolment, LE was taking lamotrigine 200 mg daily, diazepam 4.5 mg daily (slowly weaning off, but kept at a stable dose for the duration of the trial) and suvorexant for sleep. She completed a baseline questionnaire and received her first esketamine treatment in January 2024. She completed the course by mid-February having received eight esketamine treatments in total. She completed weekly questionnaires that included standard depression symptom scales, as well as daily questionnaires comprising bespoke items throughout the duration of the study. Completion of the daily questionnaires was actively monitored to ensure accurate data collection. In addition, a comprehensive post-treatment questionnaire containing the same scales used in the baseline questionnaire, was completed after 4 weeks of esketamine treatment.</p><p>The use of esketamine is relatively new and it is being trialled alongside well-established antidepressant treatments in the management of depression.<span><sup>1</sup></span> The PoET study aims to characterise the clinical profile of patients in which esketamine would be best suited, and in those that benefit, determine which antidepressants are most likely to respond to esketamine enhancement.</p><p>During esketamine treatments, LE experienced side effects such as mild dissociation and transient increased blood pressure, both of which were to be expected and resolved 1 hour after treatment administration. After week 1 of esketamine (56 mg), she reported “<i>feeling better and sleeping better</i>” (Quick Inventory of Depressive Symptoms—Clinician rated [QIDS-C] = 21). After Week 2 of esketamine (84 mg), she reported an uplift in mood immediately post treatment that was sustained for 24 h, but the effect did not remain beyond this day (QIDS-C = 14). After Week 3 of esketamine (84 mg), LE reported an uplift in her mood post treatments, and her passive suicidal ideation had completely stopped (QIDS-C = 10). After Week 4 of esketamine (84 mg), she reported a “<i>definite uplift in mood and felt hungry for the first time in a long time</i>” along with a “<i>noticeable drop in anxiety</i>”. She also noted that the effect of esketamine seems to have been sustained and she described this as “<i>[my] mood continues to remain stable and energy level is good and [I am] able to carry out necessary task[s]</i>”. LE also reported that she “<i>seem[s] to be thinking clearer and enjoy[s] some activities without thinking everything in life is a chore</i>” (QIDS-C = 6).</p><p>As per protocol, LE attended a follow-up assessment 3 weeks after the last esketamine treatment and appeared to be smiling more. She reported that she was feeling better, with a noticeable increase in motivation and capacity for exercise, and her passive suicidal ideation remained absent. She also noted that she was coping better with ongoing psychosocial stressors. While she did notice a slight drop in motivation since the last treatment, her motivation remained heightened overall as compared to baseline. Both LE's partner and her children noted her improvement, commenting that she is less tearful and is going out more. LE continues to see a psychologist and dietician regularly.</p><p>Prior to esketamine treatments, LE scored 32 on the Montgomery-Asberg Depression Rating Scale (MADRS), 17 on the Hamilton Depression rating scale (HAM-D), and 4 on the Clinical Global Impressions Scale (CGI). After 4 weeks of esketamine treatment, she scored 8, 7 and 11 on these three scales, respectively (improvements of 24, 6 and 7 points on each scale).</p><p>Figure 2 shows that overall, there was notable improvement in energy and emotion and that even with respect to cognitive functioning there was a trend towards improvement, which was modest because of a high starting point at baseline. Importantly, there is a clear decrease in anhedonia, anxiety, irritability and LE reported a sudden cessation of her passive suicidal ideation (pink shading) from day 13 onwards. Significantly, this remained absent for the remainder of the trial and 3 weeks after study completion at a follow-up assessment.</p><p>Poor or incomplete response to antidepressants is common and novel treatments and strategies are urgently needed. One approach that is widely utilised but under investigated is that of combinations of medications. Combinations of treatments are seldom studied because they do not readily lend themselves to the randomised-controlled trial (RCT) paradigm. Therefore, naturalistic studies are needed to identify those patients that respond to medications when prescribed in combination with other agents, as is often the case in real-world practice.</p><p>In this case study, we have identified some benefits from adding esketamine to lamotrigine and speculate that this may reflect either synergism or augmentation, although given it is a single case study, it has to be borne in mind that it might be neither.</p><p>The PoET study and U.L.'s position is funded by an investigator-initiated grant from Janssen-Cilag, however the authors received no funding for the writing of this article.</p><p>The authors G.S.M., U.L. and E.B. are co-investigators in the PoET Study, Clinical Trial Number: ACTRN12623001068651. G.S.M. has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier; and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. He is the recipient of an investigator-initiated grant from Janssen-Cilag (PoET Study), joint grant funding from the University of Sydney and National Taiwan University (Ignition Grant) and grant funding from The North Foundation. E.B. has received joint grant funding from the University of Sydney and National Taiwan University (Ignition Grant) and grant funding from The North Foundation. U.L. is employed through funding from an investigator-initiated grant from Janssen-Cilag for the PoET Study. C.K. referred the patient (LE) to the PoET Study.</p>\",\"PeriodicalId\":8959,\"journal\":{\"name\":\"Bipolar Disorders\",\"volume\":\"26 5\",\"pages\":\"500-504\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2024-05-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bdi.13448\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bipolar Disorders\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/bdi.13448\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bipolar Disorders","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/bdi.13448","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Adding esketamine to lamotrigine to treat major depression: Combinatorial synergism, augmentation, or neither?
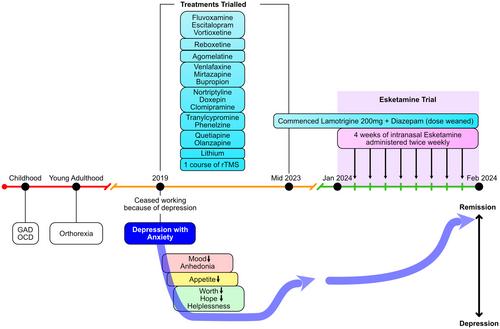
In an investigator-initiated study1 designed to determine the positioning of esketamine in the treatment (PoET) of depression, we have treated patients with severe depression. As it is a naturalistic study, we have no stipulations as to the antidepressant treatment the person is taking when commencing add-on esketamine therapy, which is administered via bi-weekly insufflation under medical supervision. Most patients that are referred are taking SSRIs, SNRIs or TCAs, and occasionally are taking MAOIs or novel agents such as vortioxetine. However, in one patient who had trialled most treatments, the physician had resorted to trialling lamotrigine even though the patient had no history of bipolar disorder, possibly because of the complexity of the illness (number of comorbidities) and lack of response.
It is this case, of a 44-year-old Caucasian female (LE) with a current psychiatric history of treatment resistant depression (TRD), along with generalized anxiety disorder (GAD), obsessive-compulsive disorder (OCD) and iatrogenic benzodiazepine dependence that we present here. Previous diagnoses also included orthorexia in recovery and substance misuse in young adulthood. Her medical history includes osteoporosis and ulcerative colitis, but she has been off steroids since 2015, and does not smoke, consume alcohol or use substances.
In late 2018, LE, then 40 years old, was diagnosed with major depressive disorder with anxiety. There was no significant precipitant for her depressive episodes and because of her illness, she stopped working in 2019. Her depressive symptoms included sadness, numbness, anhedonia, low self-worth, feelings of helplessness and hopelessness, loss of appetite, detachment and passive suicidal ideation. She described her depression as “depression with unbearable pain”, and she was “unable to see the future”. In addition to receiving psychological and dietetic treatments weekly, she also trialled multiple pharmacological treatments including SSRIs, SNRIs, TCAs, MAOIs, atypical antipsychotics and lithium augmentation (see Figure 1). She experienced a partial response with some medications but also had severe side effects. She also underwent a course of rTMS, which she reported “did nothing for me, I felt like it did less than an SSRI”.
In January 2024, the patient was referred to the CADE clinic2 and screened for PoET. After an extensive assessment process, we deemed the patient suitable for enrolment. She consented and commenced the study in January 2024. As per our protocol, she received esketamine treatments twice weekly for 4 weeks. At the time of enrolment, LE was taking lamotrigine 200 mg daily, diazepam 4.5 mg daily (slowly weaning off, but kept at a stable dose for the duration of the trial) and suvorexant for sleep. She completed a baseline questionnaire and received her first esketamine treatment in January 2024. She completed the course by mid-February having received eight esketamine treatments in total. She completed weekly questionnaires that included standard depression symptom scales, as well as daily questionnaires comprising bespoke items throughout the duration of the study. Completion of the daily questionnaires was actively monitored to ensure accurate data collection. In addition, a comprehensive post-treatment questionnaire containing the same scales used in the baseline questionnaire, was completed after 4 weeks of esketamine treatment.
The use of esketamine is relatively new and it is being trialled alongside well-established antidepressant treatments in the management of depression.1 The PoET study aims to characterise the clinical profile of patients in which esketamine would be best suited, and in those that benefit, determine which antidepressants are most likely to respond to esketamine enhancement.
During esketamine treatments, LE experienced side effects such as mild dissociation and transient increased blood pressure, both of which were to be expected and resolved 1 hour after treatment administration. After week 1 of esketamine (56 mg), she reported “feeling better and sleeping better” (Quick Inventory of Depressive Symptoms—Clinician rated [QIDS-C] = 21). After Week 2 of esketamine (84 mg), she reported an uplift in mood immediately post treatment that was sustained for 24 h, but the effect did not remain beyond this day (QIDS-C = 14). After Week 3 of esketamine (84 mg), LE reported an uplift in her mood post treatments, and her passive suicidal ideation had completely stopped (QIDS-C = 10). After Week 4 of esketamine (84 mg), she reported a “definite uplift in mood and felt hungry for the first time in a long time” along with a “noticeable drop in anxiety”. She also noted that the effect of esketamine seems to have been sustained and she described this as “[my] mood continues to remain stable and energy level is good and [I am] able to carry out necessary task[s]”. LE also reported that she “seem[s] to be thinking clearer and enjoy[s] some activities without thinking everything in life is a chore” (QIDS-C = 6).
As per protocol, LE attended a follow-up assessment 3 weeks after the last esketamine treatment and appeared to be smiling more. She reported that she was feeling better, with a noticeable increase in motivation and capacity for exercise, and her passive suicidal ideation remained absent. She also noted that she was coping better with ongoing psychosocial stressors. While she did notice a slight drop in motivation since the last treatment, her motivation remained heightened overall as compared to baseline. Both LE's partner and her children noted her improvement, commenting that she is less tearful and is going out more. LE continues to see a psychologist and dietician regularly.
Prior to esketamine treatments, LE scored 32 on the Montgomery-Asberg Depression Rating Scale (MADRS), 17 on the Hamilton Depression rating scale (HAM-D), and 4 on the Clinical Global Impressions Scale (CGI). After 4 weeks of esketamine treatment, she scored 8, 7 and 11 on these three scales, respectively (improvements of 24, 6 and 7 points on each scale).
Figure 2 shows that overall, there was notable improvement in energy and emotion and that even with respect to cognitive functioning there was a trend towards improvement, which was modest because of a high starting point at baseline. Importantly, there is a clear decrease in anhedonia, anxiety, irritability and LE reported a sudden cessation of her passive suicidal ideation (pink shading) from day 13 onwards. Significantly, this remained absent for the remainder of the trial and 3 weeks after study completion at a follow-up assessment.
Poor or incomplete response to antidepressants is common and novel treatments and strategies are urgently needed. One approach that is widely utilised but under investigated is that of combinations of medications. Combinations of treatments are seldom studied because they do not readily lend themselves to the randomised-controlled trial (RCT) paradigm. Therefore, naturalistic studies are needed to identify those patients that respond to medications when prescribed in combination with other agents, as is often the case in real-world practice.
In this case study, we have identified some benefits from adding esketamine to lamotrigine and speculate that this may reflect either synergism or augmentation, although given it is a single case study, it has to be borne in mind that it might be neither.
The PoET study and U.L.'s position is funded by an investigator-initiated grant from Janssen-Cilag, however the authors received no funding for the writing of this article.
The authors G.S.M., U.L. and E.B. are co-investigators in the PoET Study, Clinical Trial Number: ACTRN12623001068651. G.S.M. has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier; and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. He is the recipient of an investigator-initiated grant from Janssen-Cilag (PoET Study), joint grant funding from the University of Sydney and National Taiwan University (Ignition Grant) and grant funding from The North Foundation. E.B. has received joint grant funding from the University of Sydney and National Taiwan University (Ignition Grant) and grant funding from The North Foundation. U.L. is employed through funding from an investigator-initiated grant from Janssen-Cilag for the PoET Study. C.K. referred the patient (LE) to the PoET Study.
期刊介绍:
Bipolar Disorders is an international journal that publishes all research of relevance for the basic mechanisms, clinical aspects, or treatment of bipolar disorders and related illnesses. It intends to provide a single international outlet for new research in this area and covers research in the following areas:
biochemistry
physiology
neuropsychopharmacology
neuroanatomy
neuropathology
genetics
brain imaging
epidemiology
phenomenology
clinical aspects
and therapeutics of bipolar disorders
Bipolar Disorders also contains papers that form the development of new therapeutic strategies for these disorders as well as papers on the topics of schizoaffective disorders, and depressive disorders as these can be cyclic disorders with areas of overlap with bipolar disorders.
The journal will consider for publication submissions within the domain of: Perspectives, Research Articles, Correspondence, Clinical Corner, and Reflections. Within these there are a number of types of articles: invited editorials, debates, review articles, original articles, commentaries, letters to the editors, clinical conundrums, clinical curiosities, clinical care, and musings.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


