Michael S. Yule, Joshua Thompson, Khachonphat Leesahatsawat, Mariana S. Sousa, Stefan D. Anker, Jann Arends, Trude R. Balstad, Leo R. Brown, Asta Bye, Olav Dajani, Marie Fallon, Marianne J. Hjermstad, Gunnhild Jakobsen, James McDonald, Josh McGovern, Eric J. Roeland, Judith Sayers, Richard J.E. Skipworth, Inger O. Ottestad, Iain Philips, Melanie R. Simpson, Tora S. Solheim, Ola Magne Vagnildhaug, Donald McMillan, Barry J.A. Laird, Ross D. Dolan, the Cancer Cachexia Endpoints Working Group
{"title":"癌症恶病质临床试验中的生物标记终点:恶病质终点系列系统回顾 5》。","authors":"Michael S. Yule, Joshua Thompson, Khachonphat Leesahatsawat, Mariana S. Sousa, Stefan D. Anker, Jann Arends, Trude R. Balstad, Leo R. Brown, Asta Bye, Olav Dajani, Marie Fallon, Marianne J. Hjermstad, Gunnhild Jakobsen, James McDonald, Josh McGovern, Eric J. Roeland, Judith Sayers, Richard J.E. Skipworth, Inger O. Ottestad, Iain Philips, Melanie R. Simpson, Tora S. Solheim, Ola Magne Vagnildhaug, Donald McMillan, Barry J.A. Laird, Ross D. Dolan, the Cancer Cachexia Endpoints Working Group","doi":"10.1002/jcsm.13491","DOIUrl":null,"url":null,"abstract":"<p>Regulatory agencies require evidence that endpoints correlate with clinical benefit before they can be used to approve drugs. Biomarkers are often considered surrogate endpoints. In cancer cachexia trials, the measurement of biomarkers features frequently. The aim of this systematic review was to assess the frequency and diversity of biomarker endpoints in cancer cachexia trials. A comprehensive electronic literature search of MEDLINE, Embase and Cochrane (1990–2023) was completed. Eligible trials met the following criteria: adults (≥18 years), prospective design, more than 40 participants, use of a cachexia intervention for more than 14 days and use of a biomarker(s) as an endpoint. Biomarkers were defined as any objective measure that was assayed from a body fluid, including scoring systems based on these assays. Routine haematology and biochemistry to monitor intervention toxicity were not considered. Data extraction was performed using Covidence, and reporting followed PRISMA guidance (PROSPERO: CRD42022276710). A total of 5975 studies were assessed, of which 52 trials (total participants = 6522) included biomarkers as endpoints. Most studies (<i>n</i> = 29, 55.7%) included a variety of cancer types. Pharmacological interventions (<i>n</i> = 27, 51.9%) were most evaluated, followed by nutritional interventions (<i>n</i> = 20, 38.4%). Ninety-nine different biomarkers were used across the trials, and of these, 96 were assayed from blood. Albumin (<i>n</i> = 29, 55.8%) was assessed most often, followed by C-reactive protein (<i>n</i> = 22, 42.3%), interleukin-6 (<i>n</i> = 16, 30.8%) and tumour necrosis factor-α (<i>n</i> = 14, 26.9%), the latter being the only biomarker that was used to guide sample size calculations. Biomarkers were explicitly listed as a primary outcome in six trials. In total, 12 biomarkers (12.1% of 99) were used in six trials or more. Insulin-like growth factor binding protein 3 (IGFBP-3) and insulin-like growth factor 1 (IGF-1) levels both increased significantly in all three trials in which they were both used. This corresponded with a primary outcome, lean body mass, and was related to the pharmacological mechanism. Biomarkers were predominately used as exploratory rather than primary endpoints. The most commonly used biomarker, albumin, was limited by its lack of responsiveness to nutritional intervention. For a biomarker to be responsive to change, it must be related to the mechanism of action of the intervention and/or the underlying cachexia process that is modified by the intervention, as seen with IGFBP-3, IGF-1 and anamorelin. To reach regulatory approval as an endpoint, the relationship between the biomarker and clinical benefit must be clarified.</p>","PeriodicalId":48911,"journal":{"name":"Journal of Cachexia Sarcopenia and Muscle","volume":"15 3","pages":"853-867"},"PeriodicalIF":9.4000,"publicationDate":"2024-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jcsm.13491","citationCount":"0","resultStr":"{\"title\":\"Biomarker endpoints in cancer cachexia clinical trials: Systematic Review 5 of the cachexia endpoint series\",\"authors\":\"Michael S. Yule, Joshua Thompson, Khachonphat Leesahatsawat, Mariana S. Sousa, Stefan D. Anker, Jann Arends, Trude R. Balstad, Leo R. Brown, Asta Bye, Olav Dajani, Marie Fallon, Marianne J. Hjermstad, Gunnhild Jakobsen, James McDonald, Josh McGovern, Eric J. Roeland, Judith Sayers, Richard J.E. Skipworth, Inger O. Ottestad, Iain Philips, Melanie R. Simpson, Tora S. Solheim, Ola Magne Vagnildhaug, Donald McMillan, Barry J.A. Laird, Ross D. Dolan, the Cancer Cachexia Endpoints Working Group\",\"doi\":\"10.1002/jcsm.13491\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Regulatory agencies require evidence that endpoints correlate with clinical benefit before they can be used to approve drugs. Biomarkers are often considered surrogate endpoints. In cancer cachexia trials, the measurement of biomarkers features frequently. The aim of this systematic review was to assess the frequency and diversity of biomarker endpoints in cancer cachexia trials. A comprehensive electronic literature search of MEDLINE, Embase and Cochrane (1990–2023) was completed. Eligible trials met the following criteria: adults (≥18 years), prospective design, more than 40 participants, use of a cachexia intervention for more than 14 days and use of a biomarker(s) as an endpoint. Biomarkers were defined as any objective measure that was assayed from a body fluid, including scoring systems based on these assays. Routine haematology and biochemistry to monitor intervention toxicity were not considered. Data extraction was performed using Covidence, and reporting followed PRISMA guidance (PROSPERO: CRD42022276710). A total of 5975 studies were assessed, of which 52 trials (total participants = 6522) included biomarkers as endpoints. Most studies (<i>n</i> = 29, 55.7%) included a variety of cancer types. Pharmacological interventions (<i>n</i> = 27, 51.9%) were most evaluated, followed by nutritional interventions (<i>n</i> = 20, 38.4%). Ninety-nine different biomarkers were used across the trials, and of these, 96 were assayed from blood. Albumin (<i>n</i> = 29, 55.8%) was assessed most often, followed by C-reactive protein (<i>n</i> = 22, 42.3%), interleukin-6 (<i>n</i> = 16, 30.8%) and tumour necrosis factor-α (<i>n</i> = 14, 26.9%), the latter being the only biomarker that was used to guide sample size calculations. Biomarkers were explicitly listed as a primary outcome in six trials. In total, 12 biomarkers (12.1% of 99) were used in six trials or more. Insulin-like growth factor binding protein 3 (IGFBP-3) and insulin-like growth factor 1 (IGF-1) levels both increased significantly in all three trials in which they were both used. This corresponded with a primary outcome, lean body mass, and was related to the pharmacological mechanism. Biomarkers were predominately used as exploratory rather than primary endpoints. The most commonly used biomarker, albumin, was limited by its lack of responsiveness to nutritional intervention. For a biomarker to be responsive to change, it must be related to the mechanism of action of the intervention and/or the underlying cachexia process that is modified by the intervention, as seen with IGFBP-3, IGF-1 and anamorelin. To reach regulatory approval as an endpoint, the relationship between the biomarker and clinical benefit must be clarified.</p>\",\"PeriodicalId\":48911,\"journal\":{\"name\":\"Journal of Cachexia Sarcopenia and Muscle\",\"volume\":\"15 3\",\"pages\":\"853-867\"},\"PeriodicalIF\":9.4000,\"publicationDate\":\"2024-05-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jcsm.13491\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cachexia Sarcopenia and Muscle\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jcsm.13491\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cachexia Sarcopenia and Muscle","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jcsm.13491","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
Biomarker endpoints in cancer cachexia clinical trials: Systematic Review 5 of the cachexia endpoint series
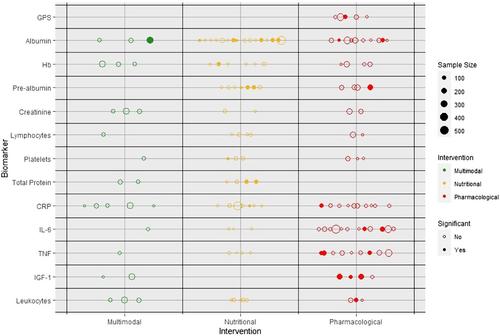
Regulatory agencies require evidence that endpoints correlate with clinical benefit before they can be used to approve drugs. Biomarkers are often considered surrogate endpoints. In cancer cachexia trials, the measurement of biomarkers features frequently. The aim of this systematic review was to assess the frequency and diversity of biomarker endpoints in cancer cachexia trials. A comprehensive electronic literature search of MEDLINE, Embase and Cochrane (1990–2023) was completed. Eligible trials met the following criteria: adults (≥18 years), prospective design, more than 40 participants, use of a cachexia intervention for more than 14 days and use of a biomarker(s) as an endpoint. Biomarkers were defined as any objective measure that was assayed from a body fluid, including scoring systems based on these assays. Routine haematology and biochemistry to monitor intervention toxicity were not considered. Data extraction was performed using Covidence, and reporting followed PRISMA guidance (PROSPERO: CRD42022276710). A total of 5975 studies were assessed, of which 52 trials (total participants = 6522) included biomarkers as endpoints. Most studies (n = 29, 55.7%) included a variety of cancer types. Pharmacological interventions (n = 27, 51.9%) were most evaluated, followed by nutritional interventions (n = 20, 38.4%). Ninety-nine different biomarkers were used across the trials, and of these, 96 were assayed from blood. Albumin (n = 29, 55.8%) was assessed most often, followed by C-reactive protein (n = 22, 42.3%), interleukin-6 (n = 16, 30.8%) and tumour necrosis factor-α (n = 14, 26.9%), the latter being the only biomarker that was used to guide sample size calculations. Biomarkers were explicitly listed as a primary outcome in six trials. In total, 12 biomarkers (12.1% of 99) were used in six trials or more. Insulin-like growth factor binding protein 3 (IGFBP-3) and insulin-like growth factor 1 (IGF-1) levels both increased significantly in all three trials in which they were both used. This corresponded with a primary outcome, lean body mass, and was related to the pharmacological mechanism. Biomarkers were predominately used as exploratory rather than primary endpoints. The most commonly used biomarker, albumin, was limited by its lack of responsiveness to nutritional intervention. For a biomarker to be responsive to change, it must be related to the mechanism of action of the intervention and/or the underlying cachexia process that is modified by the intervention, as seen with IGFBP-3, IGF-1 and anamorelin. To reach regulatory approval as an endpoint, the relationship between the biomarker and clinical benefit must be clarified.
期刊介绍:
The Journal of Cachexia, Sarcopenia and Muscle is a peer-reviewed international journal dedicated to publishing materials related to cachexia and sarcopenia, as well as body composition and its physiological and pathophysiological changes across the lifespan and in response to various illnesses from all fields of life sciences. The journal aims to provide a reliable resource for professionals interested in related research or involved in the clinical care of affected patients, such as those suffering from AIDS, cancer, chronic heart failure, chronic lung disease, liver cirrhosis, chronic kidney failure, rheumatoid arthritis, or sepsis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


