Corey Able, Brian Liao, Gal Saffati, Ankith Maremanda, James Applewhite, Ali A Nasrallah, Joseph Sonstein, Laith Alzweri, Taylor P Kohn
{"title":"为非糖尿病肥胖患者开塞马鲁肽减肥处方与勃起功能障碍风险增加有关:TriNetX 数据库研究。","authors":"Corey Able, Brian Liao, Gal Saffati, Ankith Maremanda, James Applewhite, Ali A Nasrallah, Joseph Sonstein, Laith Alzweri, Taylor P Kohn","doi":"10.1038/s41443-024-00895-6","DOIUrl":null,"url":null,"abstract":"<p><p>Semaglutide was approved in June 2021 for weight loss in non-diabetic, obese patients. While package inserts include sexual dysfunction as a side effect, no study has assessed the degree of this risk. The objective of our study is to assess the risk of developing erectile dysfunction after semaglutide is prescribed for weight loss in obese, non-diabetic men. The TriNetX Research database was used to identify men without a diagnosis of diabetes ages 18 to 50 with BMI > 30 who were prescribed semaglutide after June 1st, 2021. Men were excluded if they had a prior erectile dysfunction diagnosis, any phosphodiesterase-5 inhibitors prescription, intracavernosal injections, penile prosthesis placement, history of testosterone deficiency, testosterone prescription, pelvic radiation, radical prostatectomy, pulmonary hypertension, or were deceased. We further restricted our cohort to non-diabetic, obese men by excluding men with a prior diabetes mellitus diagnosis, a hemoglobin A1c > 6.5%, or having ever received insulin or metformin. Men were then stratified into cohorts of those that did and did not receive a semaglutide prescription. The primary outcome was the risk of new ED diagnosis and/or new prescription of phosphodiesterase type 5 inhibitors at least one month after prescription of semaglutide. The secondary outcome was risk of testosterone deficiency diagnosis. Risk was reported using risk ratios with 95% confidence intervals (95% CI). 3,094 non-diabetic, obese men ages 18-50 who received a prescription of semaglutide were identified and subsequently matched to an equal number cohort of non-diabetic, obese men who never received a prescription of semaglutide. After matching, average age at index prescription for non-diabetic, obese men was 37.8 ± 7.8 and average BMI at index prescription was 38.6 ± 5.6. Non-diabetic men prescribed semaglutide were significantly more likely to develop erectile dysfunction and/or were prescribed phosphodiesterase type 5 inhibitors (1.47% vs 0.32%; RR: 4.5; 95% CI [2.3, 9.0]) and testosterone deficiency (1.53% vs 0.80%; RR: 1.9; 95% CI [1.2, 3.1]) when compared to the control cohort of non-diabetic men who never received a semaglutide prescription.</p>","PeriodicalId":14068,"journal":{"name":"International Journal of Impotence Research","volume":" ","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2024-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Prescribing semaglutide for weight loss in non-diabetic, obese patients is associated with an increased risk of erectile dysfunction: a TriNetX database study.\",\"authors\":\"Corey Able, Brian Liao, Gal Saffati, Ankith Maremanda, James Applewhite, Ali A Nasrallah, Joseph Sonstein, Laith Alzweri, Taylor P Kohn\",\"doi\":\"10.1038/s41443-024-00895-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Semaglutide was approved in June 2021 for weight loss in non-diabetic, obese patients. While package inserts include sexual dysfunction as a side effect, no study has assessed the degree of this risk. The objective of our study is to assess the risk of developing erectile dysfunction after semaglutide is prescribed for weight loss in obese, non-diabetic men. The TriNetX Research database was used to identify men without a diagnosis of diabetes ages 18 to 50 with BMI > 30 who were prescribed semaglutide after June 1st, 2021. Men were excluded if they had a prior erectile dysfunction diagnosis, any phosphodiesterase-5 inhibitors prescription, intracavernosal injections, penile prosthesis placement, history of testosterone deficiency, testosterone prescription, pelvic radiation, radical prostatectomy, pulmonary hypertension, or were deceased. We further restricted our cohort to non-diabetic, obese men by excluding men with a prior diabetes mellitus diagnosis, a hemoglobin A1c > 6.5%, or having ever received insulin or metformin. Men were then stratified into cohorts of those that did and did not receive a semaglutide prescription. The primary outcome was the risk of new ED diagnosis and/or new prescription of phosphodiesterase type 5 inhibitors at least one month after prescription of semaglutide. The secondary outcome was risk of testosterone deficiency diagnosis. Risk was reported using risk ratios with 95% confidence intervals (95% CI). 3,094 non-diabetic, obese men ages 18-50 who received a prescription of semaglutide were identified and subsequently matched to an equal number cohort of non-diabetic, obese men who never received a prescription of semaglutide. After matching, average age at index prescription for non-diabetic, obese men was 37.8 ± 7.8 and average BMI at index prescription was 38.6 ± 5.6. Non-diabetic men prescribed semaglutide were significantly more likely to develop erectile dysfunction and/or were prescribed phosphodiesterase type 5 inhibitors (1.47% vs 0.32%; RR: 4.5; 95% CI [2.3, 9.0]) and testosterone deficiency (1.53% vs 0.80%; RR: 1.9; 95% CI [1.2, 3.1]) when compared to the control cohort of non-diabetic men who never received a semaglutide prescription.</p>\",\"PeriodicalId\":14068,\"journal\":{\"name\":\"International Journal of Impotence Research\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-05-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Impotence Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41443-024-00895-6\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Impotence Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41443-024-00895-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
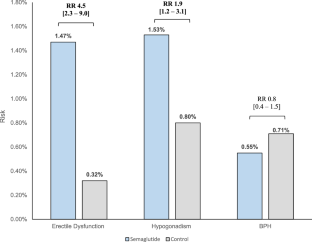
塞马鲁肽于 2021 年 6 月获批用于非糖尿病肥胖患者的减肥。虽然包装说明书中将性功能障碍列为一种副作用,但还没有研究对这种风险的程度进行评估。我们的研究目的是评估肥胖、非糖尿病男性在服用塞马鲁肽减肥后出现勃起功能障碍的风险。我们利用 TriNetX Research 数据库确定了 2021 年 6 月 1 日后处方塞马鲁肽的 18 至 50 岁、BMI>30、未确诊糖尿病的男性。如果曾诊断出勃起功能障碍、开过任何磷酸二酯酶-5 抑制剂处方、阴茎海绵体内注射、阴茎假体植入、睾酮缺乏史、睾酮处方、盆腔放射、根治性前列腺切除术、肺动脉高压或已故,则排除在外。我们进一步将队列限制为非糖尿病、肥胖男性,排除了曾被诊断为糖尿病、血红蛋白 A1c > 6.5%,或曾接受过胰岛素或二甲双胍治疗的男性。然后将获得和未获得塞马鲁肽处方的男性分层。主要结果是在开具塞马鲁肽处方后至少一个月内新诊断出ED和/或新开具5型磷酸二酯酶抑制剂处方的风险。次要结果是诊断出睾酮缺乏症的风险。风险采用风险比和 95% 置信区间 (95% CI) 进行报告。研究人员确定了 3,094 名接受过塞马鲁肽处方治疗的 18-50 岁非糖尿病肥胖男性,随后将其与从未接受过塞马鲁肽处方治疗的同等数量的非糖尿病肥胖男性进行配对。配对后,非糖尿病肥胖男性的处方指数平均年龄为 37.8 ± 7.8,处方指数平均体重指数为 38.6 ± 5.6。与从未接受过塞马鲁肽处方的非糖尿病男性对照组相比,接受过塞马鲁肽处方的非糖尿病男性出现勃起功能障碍和/或服用5型磷酸二酯酶抑制剂(1.47% vs 0.32%;RR:4.5;95% CI [2.3,9.0])和睾酮缺乏症(1.53% vs 0.80%;RR:1.9;95% CI [1.2,3.1])的几率明显更高。
Prescribing semaglutide for weight loss in non-diabetic, obese patients is associated with an increased risk of erectile dysfunction: a TriNetX database study.
Semaglutide was approved in June 2021 for weight loss in non-diabetic, obese patients. While package inserts include sexual dysfunction as a side effect, no study has assessed the degree of this risk. The objective of our study is to assess the risk of developing erectile dysfunction after semaglutide is prescribed for weight loss in obese, non-diabetic men. The TriNetX Research database was used to identify men without a diagnosis of diabetes ages 18 to 50 with BMI > 30 who were prescribed semaglutide after June 1st, 2021. Men were excluded if they had a prior erectile dysfunction diagnosis, any phosphodiesterase-5 inhibitors prescription, intracavernosal injections, penile prosthesis placement, history of testosterone deficiency, testosterone prescription, pelvic radiation, radical prostatectomy, pulmonary hypertension, or were deceased. We further restricted our cohort to non-diabetic, obese men by excluding men with a prior diabetes mellitus diagnosis, a hemoglobin A1c > 6.5%, or having ever received insulin or metformin. Men were then stratified into cohorts of those that did and did not receive a semaglutide prescription. The primary outcome was the risk of new ED diagnosis and/or new prescription of phosphodiesterase type 5 inhibitors at least one month after prescription of semaglutide. The secondary outcome was risk of testosterone deficiency diagnosis. Risk was reported using risk ratios with 95% confidence intervals (95% CI). 3,094 non-diabetic, obese men ages 18-50 who received a prescription of semaglutide were identified and subsequently matched to an equal number cohort of non-diabetic, obese men who never received a prescription of semaglutide. After matching, average age at index prescription for non-diabetic, obese men was 37.8 ± 7.8 and average BMI at index prescription was 38.6 ± 5.6. Non-diabetic men prescribed semaglutide were significantly more likely to develop erectile dysfunction and/or were prescribed phosphodiesterase type 5 inhibitors (1.47% vs 0.32%; RR: 4.5; 95% CI [2.3, 9.0]) and testosterone deficiency (1.53% vs 0.80%; RR: 1.9; 95% CI [1.2, 3.1]) when compared to the control cohort of non-diabetic men who never received a semaglutide prescription.
期刊介绍:
International Journal of Impotence Research: The Journal of Sexual Medicine addresses sexual medicine for both genders as an interdisciplinary field. This includes basic science researchers, urologists, endocrinologists, cardiologists, family practitioners, gynecologists, internists, neurologists, psychiatrists, psychologists, radiologists and other health care clinicians.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


