Andrew A Lawson, Paul Tannous, Christina Laternser, Karl Migally
{"title":"与热稀释法相比,估计菲克法系统性地高估了儿童的心脏指数。","authors":"Andrew A Lawson, Paul Tannous, Christina Laternser, Karl Migally","doi":"10.1007/s00246-024-03491-z","DOIUrl":null,"url":null,"abstract":"<p><p>Cardiac index (CI) may be derived from the Fick method, using measured or estimated oxygen consumption (VO<sub>2</sub>), or from thermodilution. In children, LaFarge VO<sub>2</sub> estimates correlate poorly with measured VO<sub>2</sub> values. In a large adult cohort, there was only modest correlation between estimated Fick CI (eFick CI) and thermodilution CI (TDCI). We evaluated the extent of agreement between eFick CI using LaFarge estimates of VO<sub>2</sub> and TDCI in a pediatric cohort. A retrospective, single-center chart review of patients 3-18 years of age who underwent cardiac catheterization with documented eFick CI and TDCI from 2004 to 2020 included 201 catheterizations from 161 unique patients. The mean patient age at catheterization was 12.2y (SD 4.4y). The most frequent diagnosis was cardiomyopathy, followed by congenital heart disease and pulmonary hypertension. TDCI and eFick CI differed by > 20% in 49% of catheterizations. eFick CI systematically exceeded TDCI by a mean percentage difference of 24% (SD 31%). Higher mean CI ((eFick CI + TDCI)/2) and older age were predictive of greater percent difference between eFick CI and TDCI. For each increase in mean CI by 1.0 L/min/m<sup>2</sup>, the expected percent difference in CI increased by 9.9% (p < 0.001). In pediatric patients undergoing cardiac catheterization, eFick CI with LaFarge VO<sub>2</sub> systematically exceeds TDCI. The difference between methods is frequently > 20%, which may have clinically significant implications. Discrepancies between eFick CI and TDCI increase at higher mean CI.</p>","PeriodicalId":19814,"journal":{"name":"Pediatric Cardiology","volume":" ","pages":"713-718"},"PeriodicalIF":1.5000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"The Estimated Fick Method Systematically Over-Estimates Cardiac Index Compared to Thermodilution in Children.\",\"authors\":\"Andrew A Lawson, Paul Tannous, Christina Laternser, Karl Migally\",\"doi\":\"10.1007/s00246-024-03491-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Cardiac index (CI) may be derived from the Fick method, using measured or estimated oxygen consumption (VO<sub>2</sub>), or from thermodilution. In children, LaFarge VO<sub>2</sub> estimates correlate poorly with measured VO<sub>2</sub> values. In a large adult cohort, there was only modest correlation between estimated Fick CI (eFick CI) and thermodilution CI (TDCI). We evaluated the extent of agreement between eFick CI using LaFarge estimates of VO<sub>2</sub> and TDCI in a pediatric cohort. A retrospective, single-center chart review of patients 3-18 years of age who underwent cardiac catheterization with documented eFick CI and TDCI from 2004 to 2020 included 201 catheterizations from 161 unique patients. The mean patient age at catheterization was 12.2y (SD 4.4y). The most frequent diagnosis was cardiomyopathy, followed by congenital heart disease and pulmonary hypertension. TDCI and eFick CI differed by > 20% in 49% of catheterizations. eFick CI systematically exceeded TDCI by a mean percentage difference of 24% (SD 31%). Higher mean CI ((eFick CI + TDCI)/2) and older age were predictive of greater percent difference between eFick CI and TDCI. For each increase in mean CI by 1.0 L/min/m<sup>2</sup>, the expected percent difference in CI increased by 9.9% (p < 0.001). In pediatric patients undergoing cardiac catheterization, eFick CI with LaFarge VO<sub>2</sub> systematically exceeds TDCI. The difference between methods is frequently > 20%, which may have clinically significant implications. Discrepancies between eFick CI and TDCI increase at higher mean CI.</p>\",\"PeriodicalId\":19814,\"journal\":{\"name\":\"Pediatric Cardiology\",\"volume\":\" \",\"pages\":\"713-718\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00246-024-03491-z\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00246-024-03491-z","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
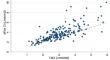
心脏指数(CI)可通过菲克法、测量或估算的耗氧量(VO2)或热稀释法得出。在儿童中,LaFarge VO2 估计值与测量的 VO2 值相关性较差。在一个大型成人队列中,估计的菲克 CI(eFick CI)与热稀释 CI(TDCI)之间的相关性不大。我们评估了儿科队列中使用 LaFarge 估算 VO2 的 eFick CI 与 TDCI 之间的一致程度。我们对 2004 年至 2020 年期间接受心导管检查并记录有 eFick CI 和 TDCI 的 3-18 岁患者进行了回顾性单中心病历审查,其中包括 161 名患者的 201 次心导管检查。患者接受导管检查时的平均年龄为 12.2 岁(标清 4.4 岁)。最常见的诊断是心肌病,其次是先天性心脏病和肺动脉高压。在 49% 的导管检查中,TDCI 和 eFick CI 的差异大于 20%。较高的平均 CI((eFick CI + TDCI)/2)和较大的年龄可预测 eFick CI 与 TDCI 之间较大的百分比差异。平均 CI 每增加 1.0 升/分钟/平方米,CI 的预期差异百分比就会增加 9.9%(p 2 系统性地超过 TDCI)。不同方法之间的差异经常大于 20%,这可能会对临床产生重大影响。平均 CI 越高,eFick CI 与 TDCI 之间的差异就越大。
The Estimated Fick Method Systematically Over-Estimates Cardiac Index Compared to Thermodilution in Children.
Cardiac index (CI) may be derived from the Fick method, using measured or estimated oxygen consumption (VO2), or from thermodilution. In children, LaFarge VO2 estimates correlate poorly with measured VO2 values. In a large adult cohort, there was only modest correlation between estimated Fick CI (eFick CI) and thermodilution CI (TDCI). We evaluated the extent of agreement between eFick CI using LaFarge estimates of VO2 and TDCI in a pediatric cohort. A retrospective, single-center chart review of patients 3-18 years of age who underwent cardiac catheterization with documented eFick CI and TDCI from 2004 to 2020 included 201 catheterizations from 161 unique patients. The mean patient age at catheterization was 12.2y (SD 4.4y). The most frequent diagnosis was cardiomyopathy, followed by congenital heart disease and pulmonary hypertension. TDCI and eFick CI differed by > 20% in 49% of catheterizations. eFick CI systematically exceeded TDCI by a mean percentage difference of 24% (SD 31%). Higher mean CI ((eFick CI + TDCI)/2) and older age were predictive of greater percent difference between eFick CI and TDCI. For each increase in mean CI by 1.0 L/min/m2, the expected percent difference in CI increased by 9.9% (p < 0.001). In pediatric patients undergoing cardiac catheterization, eFick CI with LaFarge VO2 systematically exceeds TDCI. The difference between methods is frequently > 20%, which may have clinically significant implications. Discrepancies between eFick CI and TDCI increase at higher mean CI.
期刊介绍:
The editor of Pediatric Cardiology welcomes original manuscripts concerning all aspects of heart disease in infants, children, and adolescents, including embryology and anatomy, physiology and pharmacology, biochemistry, pathology, genetics, radiology, clinical aspects, investigative cardiology, electrophysiology and echocardiography, and cardiac surgery. Articles which may include original articles, review articles, letters to the editor etc., must be written in English and must be submitted solely to Pediatric Cardiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


