Sacha Koutsikas, Antoine Yrondi, Laura Hatchondo, Rachel Debs
{"title":"回到未来:克莱因-莱文综合征可能是一种新出现的精神疾病吗?","authors":"Sacha Koutsikas, Antoine Yrondi, Laura Hatchondo, Rachel Debs","doi":"10.1111/bdi.13455","DOIUrl":null,"url":null,"abstract":"<p>Since the 20th century, atypical cases of recurrent hypersomnia are no longer related to mood disorders but are grouped together in the new Kleine-Levin syndrome (KLS).</p><p>Between neurology and psychiatry, the KLS symptoms include hypersomnia (up to 20 h of sleep/day), which may or may not be accompanied by disinhibition, derealisation, extreme apathy, cognitive dysfunction, childishness, anxiety, hallucinations, ideas of reference and delusions of grandeur. At the point of diagnosis, additional examinations (biology, imaging) are not diagnostic and are even less pathognomonic, just as is the case for psychiatric disorders.</p><p>The indication for long-term treatment based on thymoregulatory depends on the intensity and frequency of the episodes.</p><p>Today, the international literature insists on a dichotomy between BPD and very recent KLS despite the redundancy of such a distinction<span><sup>1</sup></span> (Figure 1).</p><p>KLS is commonly recognised as a neurological disease with inflammatory markers on functional imaging during episodes, between episodes and post-mortem. This has enabled it to be distinguished from mood disorders. However, recent studies on BPD have shown that it too.</p><p>In addition, studies of both patients with BPD and their relatives have found that cognitive impairment and sleep problems appear 5–6 years before the first decompensation.<span><sup>2</sup></span></p><p>At the same time, studies report that KLS leads to psychiatric decompensation in 20% of cases, with some cases being premorbid.<span><sup>3</sup></span> Following the revision of the criteria for KLS,<span><sup>4</sup></span> the number of cases being diagnosed has been increasing. Of all newly diagnosed cases of KLS, the diagnosis is in doubt in 20% of these cases, that is, in those involving latent or overt psychiatric comorbidities. These cases could, therefore, involve undiagnosed psychiatric pathologies.</p><p>While there may be doubt regarding 20% of KLS cases, 80% are genuine. The question then arises as to which symptoms are useful in diagnosis: the old triad or the new paradigm of the 2000s?</p><p>For Kleine, a neurologist, Levin, a psychiatrist, and their predecessors, it was a syndrome, not a disorder, that they were investigating. Ultimately, it was not a disorder that they were referring to, but rather an invitation for the scientific community to communicate with each other and a request for help with treatment.</p><p>Recent studies have shown that the onset of BPD is associated with frustrating and unspecific symptoms, particularly anxiety, dissociative symptoms, and issues with sleeping. The mood-related component appears much later.<span><sup>5</sup></span></p><p>One might wonder why the scientific community is resistant to the idea of classifying KLS as a mood disorder, given the heterogenic nature of bipolar spectrum disorder, which covers different types of BPD (Akiskal classification).</p><p>In practice, these are young patients who receive a quick diagnosis. Where necessary, the psychiatric diagnosis made late in adulthood is appropriate in the event of extreme psychiatric decompensation.</p><p>Whether for the 20% of KLS cases in which there is a cormorbid psychiatric pathology<span><sup>3</sup></span> or 100% of cases of KLS if the existence of such a syndrome is disproved, there is already mental health care involving child psychiatry or psychiatric monitoring for these patients.</p><p>The role of drug treatment appears to be very important. However, there are still some unanswered questions regarding its initiation early on in the course of the disease (especially in adolescents): Does it protect against severe decompensation? Does it guarantee better adherence to treatment?</p><p>Kleine-Levin Syndrome could be an emerging psychiatric disorder in the spectrum of bipolar mood disorder with its major prevention challenges as the recent nosography is debatable and clinical cases question to provide better care.</p><p>Sacha Koutsikas wrote the manuscript. Rachel Debs, Antoine Yrondi and Laura Hatchondo contributed to the manuscript, reviewed and approved the content of the final version and agreed to be responsible for all aspects of the work.</p><p>SK, RD, LH: None. AY received the speaker's honoraria from AstraZeneca, Janssen, Lundbeck, Otsuka and Servier and carried out clinical studies related to the development of Janssen and Lundbeck medicines unrelated to this work.</p><p>The violation of the Ethical Statement rules may result in severe consequences.</p><p>I agree with the above statements and declare that this submission follows the policies of Wiley Library as outlined in the Guide for Authors and in the Ethical Statement.</p>","PeriodicalId":8959,"journal":{"name":"Bipolar Disorders","volume":"26 6","pages":"617-619"},"PeriodicalIF":5.0000,"publicationDate":"2024-05-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bdi.13455","citationCount":"0","resultStr":"{\"title\":\"Back to the future: May Kleine-Levin syndrome be an emerging psychiatric disorder?\",\"authors\":\"Sacha Koutsikas, Antoine Yrondi, Laura Hatchondo, Rachel Debs\",\"doi\":\"10.1111/bdi.13455\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Since the 20th century, atypical cases of recurrent hypersomnia are no longer related to mood disorders but are grouped together in the new Kleine-Levin syndrome (KLS).</p><p>Between neurology and psychiatry, the KLS symptoms include hypersomnia (up to 20 h of sleep/day), which may or may not be accompanied by disinhibition, derealisation, extreme apathy, cognitive dysfunction, childishness, anxiety, hallucinations, ideas of reference and delusions of grandeur. At the point of diagnosis, additional examinations (biology, imaging) are not diagnostic and are even less pathognomonic, just as is the case for psychiatric disorders.</p><p>The indication for long-term treatment based on thymoregulatory depends on the intensity and frequency of the episodes.</p><p>Today, the international literature insists on a dichotomy between BPD and very recent KLS despite the redundancy of such a distinction<span><sup>1</sup></span> (Figure 1).</p><p>KLS is commonly recognised as a neurological disease with inflammatory markers on functional imaging during episodes, between episodes and post-mortem. This has enabled it to be distinguished from mood disorders. However, recent studies on BPD have shown that it too.</p><p>In addition, studies of both patients with BPD and their relatives have found that cognitive impairment and sleep problems appear 5–6 years before the first decompensation.<span><sup>2</sup></span></p><p>At the same time, studies report that KLS leads to psychiatric decompensation in 20% of cases, with some cases being premorbid.<span><sup>3</sup></span> Following the revision of the criteria for KLS,<span><sup>4</sup></span> the number of cases being diagnosed has been increasing. Of all newly diagnosed cases of KLS, the diagnosis is in doubt in 20% of these cases, that is, in those involving latent or overt psychiatric comorbidities. These cases could, therefore, involve undiagnosed psychiatric pathologies.</p><p>While there may be doubt regarding 20% of KLS cases, 80% are genuine. The question then arises as to which symptoms are useful in diagnosis: the old triad or the new paradigm of the 2000s?</p><p>For Kleine, a neurologist, Levin, a psychiatrist, and their predecessors, it was a syndrome, not a disorder, that they were investigating. Ultimately, it was not a disorder that they were referring to, but rather an invitation for the scientific community to communicate with each other and a request for help with treatment.</p><p>Recent studies have shown that the onset of BPD is associated with frustrating and unspecific symptoms, particularly anxiety, dissociative symptoms, and issues with sleeping. The mood-related component appears much later.<span><sup>5</sup></span></p><p>One might wonder why the scientific community is resistant to the idea of classifying KLS as a mood disorder, given the heterogenic nature of bipolar spectrum disorder, which covers different types of BPD (Akiskal classification).</p><p>In practice, these are young patients who receive a quick diagnosis. Where necessary, the psychiatric diagnosis made late in adulthood is appropriate in the event of extreme psychiatric decompensation.</p><p>Whether for the 20% of KLS cases in which there is a cormorbid psychiatric pathology<span><sup>3</sup></span> or 100% of cases of KLS if the existence of such a syndrome is disproved, there is already mental health care involving child psychiatry or psychiatric monitoring for these patients.</p><p>The role of drug treatment appears to be very important. However, there are still some unanswered questions regarding its initiation early on in the course of the disease (especially in adolescents): Does it protect against severe decompensation? Does it guarantee better adherence to treatment?</p><p>Kleine-Levin Syndrome could be an emerging psychiatric disorder in the spectrum of bipolar mood disorder with its major prevention challenges as the recent nosography is debatable and clinical cases question to provide better care.</p><p>Sacha Koutsikas wrote the manuscript. Rachel Debs, Antoine Yrondi and Laura Hatchondo contributed to the manuscript, reviewed and approved the content of the final version and agreed to be responsible for all aspects of the work.</p><p>SK, RD, LH: None. AY received the speaker's honoraria from AstraZeneca, Janssen, Lundbeck, Otsuka and Servier and carried out clinical studies related to the development of Janssen and Lundbeck medicines unrelated to this work.</p><p>The violation of the Ethical Statement rules may result in severe consequences.</p><p>I agree with the above statements and declare that this submission follows the policies of Wiley Library as outlined in the Guide for Authors and in the Ethical Statement.</p>\",\"PeriodicalId\":8959,\"journal\":{\"name\":\"Bipolar Disorders\",\"volume\":\"26 6\",\"pages\":\"617-619\"},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-05-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bdi.13455\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bipolar Disorders\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/bdi.13455\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bipolar Disorders","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/bdi.13455","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Back to the future: May Kleine-Levin syndrome be an emerging psychiatric disorder?
Since the 20th century, atypical cases of recurrent hypersomnia are no longer related to mood disorders but are grouped together in the new Kleine-Levin syndrome (KLS).
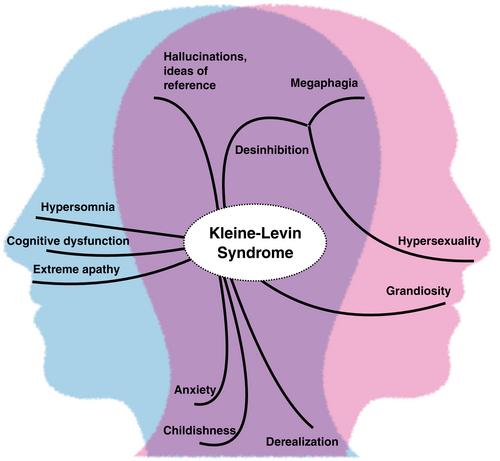
Between neurology and psychiatry, the KLS symptoms include hypersomnia (up to 20 h of sleep/day), which may or may not be accompanied by disinhibition, derealisation, extreme apathy, cognitive dysfunction, childishness, anxiety, hallucinations, ideas of reference and delusions of grandeur. At the point of diagnosis, additional examinations (biology, imaging) are not diagnostic and are even less pathognomonic, just as is the case for psychiatric disorders.
The indication for long-term treatment based on thymoregulatory depends on the intensity and frequency of the episodes.
Today, the international literature insists on a dichotomy between BPD and very recent KLS despite the redundancy of such a distinction1 (Figure 1).
KLS is commonly recognised as a neurological disease with inflammatory markers on functional imaging during episodes, between episodes and post-mortem. This has enabled it to be distinguished from mood disorders. However, recent studies on BPD have shown that it too.
In addition, studies of both patients with BPD and their relatives have found that cognitive impairment and sleep problems appear 5–6 years before the first decompensation.2
At the same time, studies report that KLS leads to psychiatric decompensation in 20% of cases, with some cases being premorbid.3 Following the revision of the criteria for KLS,4 the number of cases being diagnosed has been increasing. Of all newly diagnosed cases of KLS, the diagnosis is in doubt in 20% of these cases, that is, in those involving latent or overt psychiatric comorbidities. These cases could, therefore, involve undiagnosed psychiatric pathologies.
While there may be doubt regarding 20% of KLS cases, 80% are genuine. The question then arises as to which symptoms are useful in diagnosis: the old triad or the new paradigm of the 2000s?
For Kleine, a neurologist, Levin, a psychiatrist, and their predecessors, it was a syndrome, not a disorder, that they were investigating. Ultimately, it was not a disorder that they were referring to, but rather an invitation for the scientific community to communicate with each other and a request for help with treatment.
Recent studies have shown that the onset of BPD is associated with frustrating and unspecific symptoms, particularly anxiety, dissociative symptoms, and issues with sleeping. The mood-related component appears much later.5
One might wonder why the scientific community is resistant to the idea of classifying KLS as a mood disorder, given the heterogenic nature of bipolar spectrum disorder, which covers different types of BPD (Akiskal classification).
In practice, these are young patients who receive a quick diagnosis. Where necessary, the psychiatric diagnosis made late in adulthood is appropriate in the event of extreme psychiatric decompensation.
Whether for the 20% of KLS cases in which there is a cormorbid psychiatric pathology3 or 100% of cases of KLS if the existence of such a syndrome is disproved, there is already mental health care involving child psychiatry or psychiatric monitoring for these patients.
The role of drug treatment appears to be very important. However, there are still some unanswered questions regarding its initiation early on in the course of the disease (especially in adolescents): Does it protect against severe decompensation? Does it guarantee better adherence to treatment?
Kleine-Levin Syndrome could be an emerging psychiatric disorder in the spectrum of bipolar mood disorder with its major prevention challenges as the recent nosography is debatable and clinical cases question to provide better care.
Sacha Koutsikas wrote the manuscript. Rachel Debs, Antoine Yrondi and Laura Hatchondo contributed to the manuscript, reviewed and approved the content of the final version and agreed to be responsible for all aspects of the work.
SK, RD, LH: None. AY received the speaker's honoraria from AstraZeneca, Janssen, Lundbeck, Otsuka and Servier and carried out clinical studies related to the development of Janssen and Lundbeck medicines unrelated to this work.
The violation of the Ethical Statement rules may result in severe consequences.
I agree with the above statements and declare that this submission follows the policies of Wiley Library as outlined in the Guide for Authors and in the Ethical Statement.
期刊介绍:
Bipolar Disorders is an international journal that publishes all research of relevance for the basic mechanisms, clinical aspects, or treatment of bipolar disorders and related illnesses. It intends to provide a single international outlet for new research in this area and covers research in the following areas:
biochemistry
physiology
neuropsychopharmacology
neuroanatomy
neuropathology
genetics
brain imaging
epidemiology
phenomenology
clinical aspects
and therapeutics of bipolar disorders
Bipolar Disorders also contains papers that form the development of new therapeutic strategies for these disorders as well as papers on the topics of schizoaffective disorders, and depressive disorders as these can be cyclic disorders with areas of overlap with bipolar disorders.
The journal will consider for publication submissions within the domain of: Perspectives, Research Articles, Correspondence, Clinical Corner, and Reflections. Within these there are a number of types of articles: invited editorials, debates, review articles, original articles, commentaries, letters to the editors, clinical conundrums, clinical curiosities, clinical care, and musings.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


