R. Katie Morris, Edward Johnstone, Christoph Lees, Victoria Morton, Gordon Smith, the Royal College of Obstetricians and Gynaecologists
{"title":"小于妊娠年龄胎儿和生长受限胎儿的调查和护理(Green-top 指南第 31 号)。","authors":"R. Katie Morris, Edward Johnstone, Christoph Lees, Victoria Morton, Gordon Smith, the Royal College of Obstetricians and Gynaecologists","doi":"10.1111/1471-0528.17814","DOIUrl":null,"url":null,"abstract":"<p>The purpose of this guideline is to provide advice, based on the best evidence available, to guide clinicians regarding the investigation and care of the small-for-gestational-age (SGA) fetus and growth restricted fetus. The guideline reviews the risk factors for these conditions and provides recommendations regarding surveillance, diagnosis, and management, including recommendations for fetal monitoring and birth. Large for gestational age (LGA) is outside the scope of this guidance.</p><p>This guideline is for healthcare professionals who care for women, non-binary and trans people with a SGA fetus or with fetal growth restriction (FGR). Within this document we use the terms woman and women's health. However, it is important to acknowledge that it is not only women for whom it is necessary to access women's health and reproductive services in order to maintain their gynaecological health and reproductive wellbeing. Gynaecological and obstetric services and delivery of care must therefore be appropriate, inclusive and sensitive to the needs of those individuals whose gender identity does not align with the sex they were assigned at birth.</p><p>\n \n </p><p>Fetal size is measured at a single time point in pregnancy and assessed via individual biometric measurements (e.g. head circumference [HC], abdominal circumference [AC], and femur length [FL]) or measurements combined as estimated fetal weight (EFW) using different formulas. Fetal growth is a dynamic process occurring throughout the pregnancy requiring multiple assessments and a minimum of at least two assessments of fetal size. Additional information that can be considered includes maternal history and symptoms, amniotic fluid assessment and Doppler velocimetry. Any measurement obtained (biometry or EFW) can only be interpreted when plotted on a growth chart to determine both the centile of the measurement but also any change in growth trajectory. Growth charts are discussed further in section 7.2.1.</p><p>An appropriate for gestational age (AGA) fetus is one whose size is within a normal range for its gestational age. This is typically defined as between the 10th and 90th centiles. A fetus is considered SGA when individual biometric measurements or a combination of measurements used to estimate fetal weight fall below set parameters and requires accurate assessment of gestational age. Commonly, the definition of SGA refers to a fetus with a predicted weight or an AC measurement less than the 10th centile. SGA at birth is commonly diagnosed based on a birthweight below the 10th centile and often birthweight charts are adjusted for the sex of the baby.</p><p>FGR implies a pathological restriction of the genetic growth potential.<span><sup>1, 2</sup></span> Some, but not all, growth restricted fetuses/infants are SGA. The likelihood of FGR is higher in fetuses that are smaller.<span><sup>3</sup></span> Growth restricted fetuses may manifest evidence of fetal compromise (abnormal Doppler studies, reduced liquor volume).</p><p>Defining FGR and thus diagnosing it in a current pregnancy is challenging because of the need to determine growth potential. Similarly, risk assessing whether FGR existed in a previous pregnancy presents a different challenge. There is a need to focus on those fetuses at risk of adverse outcome and thus those that are FGR rather than SGA using varying parameters such as sequential ultrasound measurements, Doppler assessments, and biomarkers. FGR can also be subdivided clinically into early and late depending on the gestational age, with variation in gestational thresholds between 32 and 37 weeks.</p><p>A Delphi consensus-based definition of FGR (Table 1) has been suggested for use both in clinical practice and in research for early (defined in the Delphi consensus as before 32<sup>+0</sup> weeks) and late onset FGR.<span><sup>4, 5</sup></span></p><p>Saving Babies Lives Care Bundle version 3 (SBLCBv3) suggests practical definitions for FGR in a previous pregnancy, FGR in the current pregnancy, and suboptimal growth.<span><sup>6</sup></span> It highlights that absent or reversed end diastolic flow in the umbilical artery is a feature of early onset FGR, but importantly that absence of this feature (for example, a normal umbilical artery Doppler) from 32<sup>+0</sup> weeks of gestation does not mean that the fetus is not growth restricted and does not rule out the possibility of fetal compromise.</p><p>Suboptimal fetal growth may also be indicative of FGR and can be diagnosed when a previously well-grown fetus (i.e. size 10th centile or above) fails to maintain adequate fetal growth during pregnancy. Suboptimal growth is difficult to define, with SBLCBv3 defining it as a pattern of slowing growth velocity (i.e. a downward trend in the centile).<span><sup>6</sup></span> The Delphi consensus defines it as AC/EFW crossing centiles greater than two quartiles on non-customised growth centiles ≥32<sup>+0</sup> weeks (equivalent to 50 centiles).<span><sup>5</sup></span> Static growth can be defined as no forward growth velocity in EFW, or AC measured at least 14 days apart. Suboptimal fetal growth is further addressed in section 7.3.2.</p><p>Low birthweight (LBW) refers to an infant with a birthweight less than 2500 g regardless of gestation. This is no longer used in clinical practice as the majority of pregnancies have an early dating scan therefore birthweight can be adjusted for gestational age. This definition is included for interpretation of older research papers only. FGR has previously been described as symmetrical or asymmetrical and it has been proposed that it may help determine possible aetiology. However, this feature can vary and is not prognostic of outcome<span><sup>8</sup></span> so should no longer be used as a description of FGR.</p><p>Small fetuses are divided into normal (constitutionally small), non-placenta mediated growth restriction (e.g. structural, or chromosomal anomaly, inborn errors of metabolism and fetal infection), and placenta mediated growth restriction (placental dysfunction). Maternal factors such as low pre-pregnancy weight, undernutrition, substance misuse or severe anaemia can affect placental transfer of nutrients. Medical conditions can also affect placental implantation and vasculature and hence transfer (pre-eclampsia, autoimmune disease, thrombophilias, renal disease, diabetes, cardiac disease, and essential hypertension).</p><p>The underlying aetiology as well as timing of onset is important when considering the risk of adverse outcome in pregnancy. Early onset FGR is associated with significant and abnormal placentation that results in increased hypoxia and cardiovascular adaptions<span><sup>9</sup></span> and therefore carries an increased risk of adverse perinatal mortality and morbidity.<span><sup>10</sup></span> Early FGR also often coexists with maternal manifestations of placental dysfunction (hypertensive disorders of pregnancy) or maternal medical conditions and thus is easier to detect through screening pathways. In late onset FGR, the deficit in placentation is milder, with less cardiovascular adaption and a lower risk of adverse events. However, late FGR is more common, and it is more difficult to identify fetuses that may be at risk (on ultrasound scan [USS]) and thus detect, and therefore these pregnancies account for a significant proportion of adverse outcomes. They are, therefore, an important area for effective surveillance and management.</p><p>Serial symphysis fundal height (SFH) measurement is a method of surveillance for fetal size, however, it has a low sensitivity for detecting SGA/FGR fetuses.<span><sup>11</sup></span> Suspicion of a fetal growth disorder usually relies on ultrasound measurement of fetal AC or estimation of fetal weight. Care of the SGA/FGR fetus is directed at timely birth. Several surveillance tests are available, including cardiotocography (CTG), Doppler and USS to assess biophysical activity, but there is controversy about which test or combination of tests should be used to time birth in late onset FGR and SGA.</p><p>The NHS England SBLCB (a care bundle for reducing perinatal mortality) was first published in 2016 and focussed on detection and management of SGA (rather than FGR) and recommended birth at 37<sup>+0</sup> to 37<sup>+6</sup> weeks for SGA, as did the 2013 version of this RCOG guidance.<span><sup>12</sup></span> The SpiRE evaluation of the SBLCB version 1 demonstrated a measurable difference in antenatal detection of SGA babies across England.<span><sup>13</sup></span> The evaluation also demonstrated an increase in USS and inductions of labour at early term (37<sup>+0</sup>–38<sup>+6</sup> weeks). Thus, by seeking to capture all babies at risk, interventions increased in women who were only marginally at increased risk of FGR-related stillbirth, with risks to the babies of early term induction (namely increased risk of admission to the neonatal unit and potential long-term adverse effects, e.g. increased risk of special educational needs).<span><sup>14, 15</sup></span> This was partly addressed in version 2 of the bundle (2019), with different management strategies for SGA and FGR to try and reduce unnecessary intervention in SGA babies not at risk of adverse outcome.<span><sup>16</sup></span> SBLCBv3, and this guideline, addresses this further with a focus on detecting FGR and targeting intervention (i.e. birth) for those at increased risk of perinatal death.<span><sup>6</sup></span></p><p>The Cochrane Library and electronic databases (DARE, EMBASE, Trip, MEDLINE and PubMed) were searched using the relevant Medical Subject Headings (MeSH) terms, including all subheadings and synonyms, and this was combined with a keyword search and was limited to humans and English language; search terms included ‘fetal growth retardation’, ‘fetal growth restriction’ and ‘infant, small for gestational age’. The search was restricted to articles published from 2011 until December 2022. The full search strategy is available to view online as supporting information (Appendix S1 and S2). Papers identified by peer reviewers and the developers which fall outside the literature searches and may be more recent have also been included in the evidence base for the guideline.</p><p>This guideline was developed using the standard methodology for Green-top Guidelines.<span><sup>17</sup></span> Where possible, recommendations are based on available evidence. In the absence of published evidence, these have been annotated as ‘good practice points’. Further information about the assessment of evidence and the grading of recommendations may be found in Appendix I.</p><p>Risk assessment is a fundamental part of care in the maternity pathway and should be a dynamic process with continual assessment throughout the pregnancy. Risk assessment must always consider previous medical history, obstetric history and current pregnancy history with information obtained from the woman, review of medical notes and contact with previous care providers as necessary.<span><sup>18</sup></span> All pregnant women should have a risk assessment for FGR carried out by 14 weeks of gestation using an agreed pathway.<span><sup>6</sup></span></p><p>The likelihood of a FGR or FGR-related stillbirth occurring in a pregnancy is influenced by many factors. When considering risk assessment, the following are important: <i>a priori</i> risk (this is the probability of an event occurring that the woman has as she enters the pregnancy based on previous history); absence of risk factors (e.g. if a certain risk factor is not present does this reduce the risk overall and the influence of other risk factors that are present); if multiple risk factors are present how do these interplay and change the level of risk. This information is not known in sufficient detail for many conditions in pregnancy nor related to risk factors for FGR.</p><p>Risk assessment in FGR is also challenged by the fact that many analyses of risk factors for fetal growth disorders identify newborns with a birthweight less than the 10th centile as a proxy for FGR, with the majority of these births occurring at term and thus including a significant proportion of heathy smaller babies. Hence, studies using SGA as a proxy for FGR may underestimate the risk of adverse outcomes associated with FGR. This makes evidence assimilation difficult to identify which women should have increased surveillance.</p><p>There have been several risk assessment models designed for the prediction of pre-eclampsia that have been used for SGA prediction. There are data from the ASPRE randomised controlled trial (RCT; model for prediction of pre-eclampsia and aspirin administration) and SPREE study (prediction of pre-eclampsia) related to SGA prediction that identifies a high proportion of cases of preterm SGA that can be prevented by the prophylactic use of aspirin.<span><sup>19</sup></span> As these models are designed for pre-eclampsia prediction, they can be expected to have utility in prediction of FGR associated with placental dysfunction and pre-eclampsia but cannot assess all risk factors for FGR. These are discussed further in section 5.2.4.</p><p>Tools used to assess risk should provide a structured, consistent approach that can adapt throughout the pregnancy and support the pregnant woman and her clinician in making decisions about her care by making personalised care recommendations using clinically validated machine learning algorithms. Checklists for the presence of risk factors cannot weigh or assess this interaction between risk factors as described above, they also address risk as a binary function of present or absent and cannot consider all the information available from the presence and “level” of the risk. They also do not provide information in a way that can support decision making. Thus, it is imperative that future research addresses development of prediction models that are designed specifically for FGR and importantly FGR with adverse outcome, so that they can be incorporated into tools such as the Tommy's App,<span><sup>20</sup></span> a clinical decision tool being developed by Tommy's and the RCOG and other electronic patient record systems.</p><p>Within this section, the known risk factors for FGR and relevant evidence are discussed. A pathway for assessing risk and subsequent management is shown in Appendix II. It is recognised that this pathway has some of the limitations of the checklist approach as discussed above. However, this pathway attempts to incorporate all the risk factors detailed below for FGR and provide an assessment of level of risk in keeping with the National Institute for Health and Care Excellence (NICE) guideline [CG62] for pathways of care.<span><sup>18</sup></span> It is recognised that maternity providers may wish to use technology platforms and validated prediction models for pre-eclampsia and placental dysfunction prediction. Where this is the case, providers must ensure that risk assessment for other FGR risks not related to pre-eclampsia can be facilitated.</p><p>Women must also be assessed at booking for conditions where SFH measurements are not appropriate (e.g. raised body mass index [BMI] of 35 kg/m<sup>2</sup> or above at booking; presence of fibroids in uterus [based on clinical judgement]).</p><p>The risks of a pregnant woman developing early or late onset FGR are strongly linked to concurrent pregnancy risk factors. As a result of this, the prevalence of FGR varies dramatically in different pregnant populations directly influencing the performance of prediction and detection methods. Early onset FGR is a relatively uncommon condition (~0.3%) with late onset FGR being more common.</p><p>\n \n </p><p>Historically, identification of severe SGA (either EFW below the 3rd or 5th centile) was used as a marker for aneuploidy and studies which predated widespread population based screening for aneuploidy reported aneuploidy rates of up to 20%.<span><sup>286-288</sup></span> These data are less applicable in modern practice, because of the widespread use of population-based screening for aneuploidy. However, invasive testing should be considered in the context of severe SGA because of the possibility of other chromosomal abnormalities which can be detected using DNA microarrays. A systematic review and meta-analysis demonstrated that in fetuses undergoing invasive testing for FGR with no other structural anomalies there was a 4% incremental yield of chromosomal microarray analysis (CMA) over karyotyping and a 10% incremental yield in FGR with associated fetal malformations.<span><sup>289</sup></span> <i>[Evidence level 2++]</i></p><p>Prenatal exome sequencing has limited incremental yield over standard karyotyping and microarray in fetuses with isolated FGR. <i>[Evidence 2++]</i></p><p>A large population-based study from Israel reported a 3% detection rate of pathological abnormalities using microarray in the context of FGR, and only a single case out of 13 was an aneuploidy, underlining the transformative effect of population screening for aneuploidy on this association.<span><sup>290</sup></span> Therefore, when invasive testing is undertaken in the context of SGA fetal biometry, analysis of specimens should include CMA for the detection of microdeletions and microinsertions. In early onset FGR CMA demonstrated an incremental yield over karyotyping of 4.8% in isolated FGR, 10% in FGR with non-structural anomalies and 10.5% in FGR with structural anomalies.<span><sup>291</sup></span> <i>[Evidence level 2+]</i></p><p>A retrospective cohort study reported the associations with a below the 5th centile FL at the time of a 17–22-week anomaly scan (with or without other features).<span><sup>292</sup></span> The positive likelihood ratio for trisomy 21 was 8.8, for 13/18 it was 6.5 and for other unbalanced structural chromosomal abnormalities it was 17.4, with an absolute risk of 1 in 339. There was an approximate four-fold subsequent risk of both PTB and birth of an SGA infant. This has been confirmed in a systematic review, which demonstrated that an isolated short FL is significantly associated with SGA (OR 4.04, 95% CI 3.63–4.50) and PTB (OR 3.09, 95% CI 1.57–6.08).<span><sup>293</sup></span> <i>[Evidence level 2++]</i></p><p>A case series of 158 fetuses with an AC of the 5th centile or below during a detailed scan at 18–24 weeks (isolated feature) demonstrated two cases of trisomy 21 and a single case of an unbalanced structural chromosomal abnormality (detected by SNP array).<span><sup>294</sup></span> <i>[Evidence level 2–]</i></p><p>Hence, invasive diagnostic testing (amniocentesis, fetal blood sampling or placental biopsy/chorionic villus sampling) should be offered in severely SGA fetuses with structural anomalies and considered in non-anomalous fetuses detected before 23 weeks of gestation, especially if uterine artery Doppler is normal.</p><p>Follow-up scans should also be arranged given the association with subsequent birth of an SGA infant and the timing of commencement and frequency individualised following the additional investigations.</p><p>Fetal infections are responsible for up to 5% of SGA fetuses.<span><sup>295</sup></span> The most common pathogens are reported to be cytomegalovirus (CMV), toxoplasmosis, malaria and syphilis, although a multicentre study found no association between congenital toxoplasmosis and incidence of a SGA infant.<span><sup>295, 296</sup></span> A full maternal TORCH screen is unnecessary and testing should be based on history and presentation.<span><sup>297</sup></span> Malaria is a significant cause of PTB and LBW worldwide and it should be considered in those from, or who have travelled in, endemic areas.<span><sup>298</sup></span> In congenital Zika virus infection, FGR is seen in 10% of affected pregnancies, and a femur-sparing pattern of FGR is commonly seen.<span><sup>299</sup></span> <i>[Evidence level 2–]</i></p><p>\n \n </p><p>There are no proven interventions in SGA and FGR other than birth of the baby. Experimental treatments under investigation in early phase clinical trials/studies include maternal VEGF (vascular endothelial growth factor) gene therapy, melatonin and for pre-eclampsia with the potential to impact on fetal growth; statins, nitric oxide donors, proton pump inhibitors and N-acetycysteine. Preclinical investigations are underway in nanoparticles, microRNAs, hydrogen sulphide and creatinine.<span><sup>300</sup></span></p><p>PDE5 inhibitors have been tested in women with early onset placental disease, including FGR pregnancies to determine if they can improve outcomes. Most studies have focused on sildenafil (Viagra) which was shown to improve Doppler parameters in animal models and suggested in case series to be effective in increasing human fetal growth velocity.<span><sup>301, 302</sup></span> A small RCT of sildenafil (50 mg three times daily [TDS]) in women with early onset pre-eclampsia reported a prolongation of pregnancy by 4 days, although only 60% of participants had recorded SGA and there was no effect of treatment on birthweight.<span><sup>303</sup></span> However, prospective RCTs focusing on FGR have failed to show any benefit. Results from the international STRIDER collaboration did not show any prolongation in pregnancy or improvement in outcome from sildenafil (25 mg TDS) treatment.<span><sup>304, 305</sup></span> The Dutch arm of STRIDER study was stopped early because of safety concerns, although meta-analysis of outcomes from the three studies has failed to show a conclusively detrimental effect.<span><sup>306</sup></span> Tadalafil, a longer acting PDE5 inhibitor has also been tested in case reports with reported improved neonatal outcome and no adverse effects, but no RCT evidence is currently available.<span><sup>307, 308</sup></span> Therefore although some studies have suggested benefit using PDE5 inhibitors to improve outcomes in FGR pregnancies, the negative results from STRIDER do not support the use of these drugs outside of clinical trials for the treatment or prevention of FGR. <i>[Evidence level 1+]</i></p><p>RCT evidence does not support the use of LMWH as an effective treatment to prevent SGA or FGR, even in the presence of heritable thrombophilia, and should only be used in women at risk of thromboembolic disease.<span><sup>157, 158, 160, 161</sup></span> There is insufficient evidence that administration of LMWH to pregnancies with FGR prolongs or improves pregnancy outcome.<span><sup>309</sup></span> <i>[Evidence level 1++]</i></p><p>The birth of a preterm, or early term newborn, based on concerns regarding fetal growth should be optimised. Caring for women and babies at the time of an extremely premature birth is challenging. Detailed guidance is provided by the British Association of Perinatal Medicine (BAPM).<span><sup>354</sup></span> This section refers to recommendations for perinatal optimisation when active care is planned for the birth of a baby with FGR. The care of babies at 22<sup>+0</sup>–23<sup>+6</sup> weeks of gestation is particularly challenging and parents must be supported by personalised counselling to help them decide how they wish their baby to be cared for as detailed in the BAPM framework.</p><p>\n \n </p><p>As discussed in section 4, the birth of a baby with FGR is a major risk factor for FGR in a subsequent pregnancy and the postnatal period offers an opportunity to address modifiable risk factors. The most important of these is reducing exposure to second-hand smoke. NICE guideline [NG209] recommends that maternity services establish links with contraceptive services, fertility clinics and antenatal and postnatal services so that everyone working in those organisations knows about local stop-smoking support. This will reduce the risk of newborn babies being exposed to second-hand smoke and reduce the number of women going into their next pregnancy as a smoker.<span><sup>83</sup></span></p><p>Following the birth of a baby with FGR, investigations should be offered to try to determine the underlying cause and help provide an opportunity to discuss risk of recurrence and possible interventions to reduce risk at a prepregnancy appointment. These investigations should consider placental histopathology which may be useful<span><sup>372</sup></span> (as recommended by the Royal College of Pathologists defined as birthweight below the 10<sup>th</sup> centile with an abnormal fetal growth curve) and investigation for acquired thrombophilias.<span><sup>373</sup></span> <i>[Evidence level 2–]</i></p><p>Modifiable risk factors should be addressed such as lifestyle factors (e.g. smoking, BMI) and medical conditions optimised. Plans for prevention (i.e. aspirin) and monitoring in future pregnancies should be discussed.</p><p>None.</p><p>All those involved in the development of the Green-top Guidelines, including the Guidelines Committee, Guidelines Committee co-chairs, guideline developers, peer reviewers and other reviewers, are unpaid volunteers and receive no direct funding for their work in producing the guideline. The exception to this are the RCOG staff involved who are salaried employees of the College and Guidelines Committee members who receive reimbursement for expenses for attending Guidelines Committee meetings. Please see more information on travel expense rules on the RCOG website.</p><p>RKM is the chair of the RCOG Scientific Advisory Committee, Deputy National Specialty Lead for Reproductive Health and Childbirth Clinical Research Network NIHR and President of the British Maternal Fetal Medicine Society. EJ received a NERC RESPIRE grant. CL is chief investigator of the TRUFFLE 2 study of moderate preterm fetal growth restriction and has received NIHR HTA funding to Imperial College London. VM has declared no conflicts of interest. GS has received the following funding, paid to their institution: contract from Wellcome Leap for maternal serum proteomics to understand and to predict pregnancy complications leading to stillbirth, contract from Roche Diagnostics Ltd. For an Investigator Initiated Study Agreement: Pregnancy Outcome Prediction Study 2; grants from MRC for pre-labour invasion of the human uterus by Streptococcus agalactiae, from the Wellcome Trust for the evaluation and development of novel diagnostic methods to understand and prevent placentally-related complications of human pregnancy, from the NIHR Cambridge Biomedical Research Centre as Theme Leader for Women's Health and Paediatrics and from the MRC for a quantitative serum metabolite ratio to predict fetal growth abnormalities. They have also personally received a consulting fee from GSK as consultant and member of expert panel for RSV vaccination in pregnancy.</p><p>None.</p>","PeriodicalId":50729,"journal":{"name":"Bjog-An International Journal of Obstetrics and Gynaecology","volume":"131 9","pages":"e31-e80"},"PeriodicalIF":4.3000,"publicationDate":"2024-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1471-0528.17814","citationCount":"0","resultStr":"{\"title\":\"Investigation and Care of a Small-for-Gestational-Age Fetus and a Growth Restricted Fetus (Green-top Guideline No. 31)\",\"authors\":\"R. Katie Morris, Edward Johnstone, Christoph Lees, Victoria Morton, Gordon Smith, the Royal College of Obstetricians and Gynaecologists\",\"doi\":\"10.1111/1471-0528.17814\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The purpose of this guideline is to provide advice, based on the best evidence available, to guide clinicians regarding the investigation and care of the small-for-gestational-age (SGA) fetus and growth restricted fetus. The guideline reviews the risk factors for these conditions and provides recommendations regarding surveillance, diagnosis, and management, including recommendations for fetal monitoring and birth. Large for gestational age (LGA) is outside the scope of this guidance.</p><p>This guideline is for healthcare professionals who care for women, non-binary and trans people with a SGA fetus or with fetal growth restriction (FGR). Within this document we use the terms woman and women's health. However, it is important to acknowledge that it is not only women for whom it is necessary to access women's health and reproductive services in order to maintain their gynaecological health and reproductive wellbeing. Gynaecological and obstetric services and delivery of care must therefore be appropriate, inclusive and sensitive to the needs of those individuals whose gender identity does not align with the sex they were assigned at birth.</p><p>\\n \\n </p><p>Fetal size is measured at a single time point in pregnancy and assessed via individual biometric measurements (e.g. head circumference [HC], abdominal circumference [AC], and femur length [FL]) or measurements combined as estimated fetal weight (EFW) using different formulas. Fetal growth is a dynamic process occurring throughout the pregnancy requiring multiple assessments and a minimum of at least two assessments of fetal size. Additional information that can be considered includes maternal history and symptoms, amniotic fluid assessment and Doppler velocimetry. Any measurement obtained (biometry or EFW) can only be interpreted when plotted on a growth chart to determine both the centile of the measurement but also any change in growth trajectory. Growth charts are discussed further in section 7.2.1.</p><p>An appropriate for gestational age (AGA) fetus is one whose size is within a normal range for its gestational age. This is typically defined as between the 10th and 90th centiles. A fetus is considered SGA when individual biometric measurements or a combination of measurements used to estimate fetal weight fall below set parameters and requires accurate assessment of gestational age. Commonly, the definition of SGA refers to a fetus with a predicted weight or an AC measurement less than the 10th centile. SGA at birth is commonly diagnosed based on a birthweight below the 10th centile and often birthweight charts are adjusted for the sex of the baby.</p><p>FGR implies a pathological restriction of the genetic growth potential.<span><sup>1, 2</sup></span> Some, but not all, growth restricted fetuses/infants are SGA. The likelihood of FGR is higher in fetuses that are smaller.<span><sup>3</sup></span> Growth restricted fetuses may manifest evidence of fetal compromise (abnormal Doppler studies, reduced liquor volume).</p><p>Defining FGR and thus diagnosing it in a current pregnancy is challenging because of the need to determine growth potential. Similarly, risk assessing whether FGR existed in a previous pregnancy presents a different challenge. There is a need to focus on those fetuses at risk of adverse outcome and thus those that are FGR rather than SGA using varying parameters such as sequential ultrasound measurements, Doppler assessments, and biomarkers. FGR can also be subdivided clinically into early and late depending on the gestational age, with variation in gestational thresholds between 32 and 37 weeks.</p><p>A Delphi consensus-based definition of FGR (Table 1) has been suggested for use both in clinical practice and in research for early (defined in the Delphi consensus as before 32<sup>+0</sup> weeks) and late onset FGR.<span><sup>4, 5</sup></span></p><p>Saving Babies Lives Care Bundle version 3 (SBLCBv3) suggests practical definitions for FGR in a previous pregnancy, FGR in the current pregnancy, and suboptimal growth.<span><sup>6</sup></span> It highlights that absent or reversed end diastolic flow in the umbilical artery is a feature of early onset FGR, but importantly that absence of this feature (for example, a normal umbilical artery Doppler) from 32<sup>+0</sup> weeks of gestation does not mean that the fetus is not growth restricted and does not rule out the possibility of fetal compromise.</p><p>Suboptimal fetal growth may also be indicative of FGR and can be diagnosed when a previously well-grown fetus (i.e. size 10th centile or above) fails to maintain adequate fetal growth during pregnancy. Suboptimal growth is difficult to define, with SBLCBv3 defining it as a pattern of slowing growth velocity (i.e. a downward trend in the centile).<span><sup>6</sup></span> The Delphi consensus defines it as AC/EFW crossing centiles greater than two quartiles on non-customised growth centiles ≥32<sup>+0</sup> weeks (equivalent to 50 centiles).<span><sup>5</sup></span> Static growth can be defined as no forward growth velocity in EFW, or AC measured at least 14 days apart. Suboptimal fetal growth is further addressed in section 7.3.2.</p><p>Low birthweight (LBW) refers to an infant with a birthweight less than 2500 g regardless of gestation. This is no longer used in clinical practice as the majority of pregnancies have an early dating scan therefore birthweight can be adjusted for gestational age. This definition is included for interpretation of older research papers only. FGR has previously been described as symmetrical or asymmetrical and it has been proposed that it may help determine possible aetiology. However, this feature can vary and is not prognostic of outcome<span><sup>8</sup></span> so should no longer be used as a description of FGR.</p><p>Small fetuses are divided into normal (constitutionally small), non-placenta mediated growth restriction (e.g. structural, or chromosomal anomaly, inborn errors of metabolism and fetal infection), and placenta mediated growth restriction (placental dysfunction). Maternal factors such as low pre-pregnancy weight, undernutrition, substance misuse or severe anaemia can affect placental transfer of nutrients. Medical conditions can also affect placental implantation and vasculature and hence transfer (pre-eclampsia, autoimmune disease, thrombophilias, renal disease, diabetes, cardiac disease, and essential hypertension).</p><p>The underlying aetiology as well as timing of onset is important when considering the risk of adverse outcome in pregnancy. Early onset FGR is associated with significant and abnormal placentation that results in increased hypoxia and cardiovascular adaptions<span><sup>9</sup></span> and therefore carries an increased risk of adverse perinatal mortality and morbidity.<span><sup>10</sup></span> Early FGR also often coexists with maternal manifestations of placental dysfunction (hypertensive disorders of pregnancy) or maternal medical conditions and thus is easier to detect through screening pathways. In late onset FGR, the deficit in placentation is milder, with less cardiovascular adaption and a lower risk of adverse events. However, late FGR is more common, and it is more difficult to identify fetuses that may be at risk (on ultrasound scan [USS]) and thus detect, and therefore these pregnancies account for a significant proportion of adverse outcomes. They are, therefore, an important area for effective surveillance and management.</p><p>Serial symphysis fundal height (SFH) measurement is a method of surveillance for fetal size, however, it has a low sensitivity for detecting SGA/FGR fetuses.<span><sup>11</sup></span> Suspicion of a fetal growth disorder usually relies on ultrasound measurement of fetal AC or estimation of fetal weight. Care of the SGA/FGR fetus is directed at timely birth. Several surveillance tests are available, including cardiotocography (CTG), Doppler and USS to assess biophysical activity, but there is controversy about which test or combination of tests should be used to time birth in late onset FGR and SGA.</p><p>The NHS England SBLCB (a care bundle for reducing perinatal mortality) was first published in 2016 and focussed on detection and management of SGA (rather than FGR) and recommended birth at 37<sup>+0</sup> to 37<sup>+6</sup> weeks for SGA, as did the 2013 version of this RCOG guidance.<span><sup>12</sup></span> The SpiRE evaluation of the SBLCB version 1 demonstrated a measurable difference in antenatal detection of SGA babies across England.<span><sup>13</sup></span> The evaluation also demonstrated an increase in USS and inductions of labour at early term (37<sup>+0</sup>–38<sup>+6</sup> weeks). Thus, by seeking to capture all babies at risk, interventions increased in women who were only marginally at increased risk of FGR-related stillbirth, with risks to the babies of early term induction (namely increased risk of admission to the neonatal unit and potential long-term adverse effects, e.g. increased risk of special educational needs).<span><sup>14, 15</sup></span> This was partly addressed in version 2 of the bundle (2019), with different management strategies for SGA and FGR to try and reduce unnecessary intervention in SGA babies not at risk of adverse outcome.<span><sup>16</sup></span> SBLCBv3, and this guideline, addresses this further with a focus on detecting FGR and targeting intervention (i.e. birth) for those at increased risk of perinatal death.<span><sup>6</sup></span></p><p>The Cochrane Library and electronic databases (DARE, EMBASE, Trip, MEDLINE and PubMed) were searched using the relevant Medical Subject Headings (MeSH) terms, including all subheadings and synonyms, and this was combined with a keyword search and was limited to humans and English language; search terms included ‘fetal growth retardation’, ‘fetal growth restriction’ and ‘infant, small for gestational age’. The search was restricted to articles published from 2011 until December 2022. The full search strategy is available to view online as supporting information (Appendix S1 and S2). Papers identified by peer reviewers and the developers which fall outside the literature searches and may be more recent have also been included in the evidence base for the guideline.</p><p>This guideline was developed using the standard methodology for Green-top Guidelines.<span><sup>17</sup></span> Where possible, recommendations are based on available evidence. In the absence of published evidence, these have been annotated as ‘good practice points’. Further information about the assessment of evidence and the grading of recommendations may be found in Appendix I.</p><p>Risk assessment is a fundamental part of care in the maternity pathway and should be a dynamic process with continual assessment throughout the pregnancy. Risk assessment must always consider previous medical history, obstetric history and current pregnancy history with information obtained from the woman, review of medical notes and contact with previous care providers as necessary.<span><sup>18</sup></span> All pregnant women should have a risk assessment for FGR carried out by 14 weeks of gestation using an agreed pathway.<span><sup>6</sup></span></p><p>The likelihood of a FGR or FGR-related stillbirth occurring in a pregnancy is influenced by many factors. When considering risk assessment, the following are important: <i>a priori</i> risk (this is the probability of an event occurring that the woman has as she enters the pregnancy based on previous history); absence of risk factors (e.g. if a certain risk factor is not present does this reduce the risk overall and the influence of other risk factors that are present); if multiple risk factors are present how do these interplay and change the level of risk. This information is not known in sufficient detail for many conditions in pregnancy nor related to risk factors for FGR.</p><p>Risk assessment in FGR is also challenged by the fact that many analyses of risk factors for fetal growth disorders identify newborns with a birthweight less than the 10th centile as a proxy for FGR, with the majority of these births occurring at term and thus including a significant proportion of heathy smaller babies. Hence, studies using SGA as a proxy for FGR may underestimate the risk of adverse outcomes associated with FGR. This makes evidence assimilation difficult to identify which women should have increased surveillance.</p><p>There have been several risk assessment models designed for the prediction of pre-eclampsia that have been used for SGA prediction. There are data from the ASPRE randomised controlled trial (RCT; model for prediction of pre-eclampsia and aspirin administration) and SPREE study (prediction of pre-eclampsia) related to SGA prediction that identifies a high proportion of cases of preterm SGA that can be prevented by the prophylactic use of aspirin.<span><sup>19</sup></span> As these models are designed for pre-eclampsia prediction, they can be expected to have utility in prediction of FGR associated with placental dysfunction and pre-eclampsia but cannot assess all risk factors for FGR. These are discussed further in section 5.2.4.</p><p>Tools used to assess risk should provide a structured, consistent approach that can adapt throughout the pregnancy and support the pregnant woman and her clinician in making decisions about her care by making personalised care recommendations using clinically validated machine learning algorithms. Checklists for the presence of risk factors cannot weigh or assess this interaction between risk factors as described above, they also address risk as a binary function of present or absent and cannot consider all the information available from the presence and “level” of the risk. They also do not provide information in a way that can support decision making. Thus, it is imperative that future research addresses development of prediction models that are designed specifically for FGR and importantly FGR with adverse outcome, so that they can be incorporated into tools such as the Tommy's App,<span><sup>20</sup></span> a clinical decision tool being developed by Tommy's and the RCOG and other electronic patient record systems.</p><p>Within this section, the known risk factors for FGR and relevant evidence are discussed. A pathway for assessing risk and subsequent management is shown in Appendix II. It is recognised that this pathway has some of the limitations of the checklist approach as discussed above. However, this pathway attempts to incorporate all the risk factors detailed below for FGR and provide an assessment of level of risk in keeping with the National Institute for Health and Care Excellence (NICE) guideline [CG62] for pathways of care.<span><sup>18</sup></span> It is recognised that maternity providers may wish to use technology platforms and validated prediction models for pre-eclampsia and placental dysfunction prediction. Where this is the case, providers must ensure that risk assessment for other FGR risks not related to pre-eclampsia can be facilitated.</p><p>Women must also be assessed at booking for conditions where SFH measurements are not appropriate (e.g. raised body mass index [BMI] of 35 kg/m<sup>2</sup> or above at booking; presence of fibroids in uterus [based on clinical judgement]).</p><p>The risks of a pregnant woman developing early or late onset FGR are strongly linked to concurrent pregnancy risk factors. As a result of this, the prevalence of FGR varies dramatically in different pregnant populations directly influencing the performance of prediction and detection methods. Early onset FGR is a relatively uncommon condition (~0.3%) with late onset FGR being more common.</p><p>\\n \\n </p><p>Historically, identification of severe SGA (either EFW below the 3rd or 5th centile) was used as a marker for aneuploidy and studies which predated widespread population based screening for aneuploidy reported aneuploidy rates of up to 20%.<span><sup>286-288</sup></span> These data are less applicable in modern practice, because of the widespread use of population-based screening for aneuploidy. However, invasive testing should be considered in the context of severe SGA because of the possibility of other chromosomal abnormalities which can be detected using DNA microarrays. A systematic review and meta-analysis demonstrated that in fetuses undergoing invasive testing for FGR with no other structural anomalies there was a 4% incremental yield of chromosomal microarray analysis (CMA) over karyotyping and a 10% incremental yield in FGR with associated fetal malformations.<span><sup>289</sup></span> <i>[Evidence level 2++]</i></p><p>Prenatal exome sequencing has limited incremental yield over standard karyotyping and microarray in fetuses with isolated FGR. <i>[Evidence 2++]</i></p><p>A large population-based study from Israel reported a 3% detection rate of pathological abnormalities using microarray in the context of FGR, and only a single case out of 13 was an aneuploidy, underlining the transformative effect of population screening for aneuploidy on this association.<span><sup>290</sup></span> Therefore, when invasive testing is undertaken in the context of SGA fetal biometry, analysis of specimens should include CMA for the detection of microdeletions and microinsertions. In early onset FGR CMA demonstrated an incremental yield over karyotyping of 4.8% in isolated FGR, 10% in FGR with non-structural anomalies and 10.5% in FGR with structural anomalies.<span><sup>291</sup></span> <i>[Evidence level 2+]</i></p><p>A retrospective cohort study reported the associations with a below the 5th centile FL at the time of a 17–22-week anomaly scan (with or without other features).<span><sup>292</sup></span> The positive likelihood ratio for trisomy 21 was 8.8, for 13/18 it was 6.5 and for other unbalanced structural chromosomal abnormalities it was 17.4, with an absolute risk of 1 in 339. There was an approximate four-fold subsequent risk of both PTB and birth of an SGA infant. This has been confirmed in a systematic review, which demonstrated that an isolated short FL is significantly associated with SGA (OR 4.04, 95% CI 3.63–4.50) and PTB (OR 3.09, 95% CI 1.57–6.08).<span><sup>293</sup></span> <i>[Evidence level 2++]</i></p><p>A case series of 158 fetuses with an AC of the 5th centile or below during a detailed scan at 18–24 weeks (isolated feature) demonstrated two cases of trisomy 21 and a single case of an unbalanced structural chromosomal abnormality (detected by SNP array).<span><sup>294</sup></span> <i>[Evidence level 2–]</i></p><p>Hence, invasive diagnostic testing (amniocentesis, fetal blood sampling or placental biopsy/chorionic villus sampling) should be offered in severely SGA fetuses with structural anomalies and considered in non-anomalous fetuses detected before 23 weeks of gestation, especially if uterine artery Doppler is normal.</p><p>Follow-up scans should also be arranged given the association with subsequent birth of an SGA infant and the timing of commencement and frequency individualised following the additional investigations.</p><p>Fetal infections are responsible for up to 5% of SGA fetuses.<span><sup>295</sup></span> The most common pathogens are reported to be cytomegalovirus (CMV), toxoplasmosis, malaria and syphilis, although a multicentre study found no association between congenital toxoplasmosis and incidence of a SGA infant.<span><sup>295, 296</sup></span> A full maternal TORCH screen is unnecessary and testing should be based on history and presentation.<span><sup>297</sup></span> Malaria is a significant cause of PTB and LBW worldwide and it should be considered in those from, or who have travelled in, endemic areas.<span><sup>298</sup></span> In congenital Zika virus infection, FGR is seen in 10% of affected pregnancies, and a femur-sparing pattern of FGR is commonly seen.<span><sup>299</sup></span> <i>[Evidence level 2–]</i></p><p>\\n \\n </p><p>There are no proven interventions in SGA and FGR other than birth of the baby. Experimental treatments under investigation in early phase clinical trials/studies include maternal VEGF (vascular endothelial growth factor) gene therapy, melatonin and for pre-eclampsia with the potential to impact on fetal growth; statins, nitric oxide donors, proton pump inhibitors and N-acetycysteine. Preclinical investigations are underway in nanoparticles, microRNAs, hydrogen sulphide and creatinine.<span><sup>300</sup></span></p><p>PDE5 inhibitors have been tested in women with early onset placental disease, including FGR pregnancies to determine if they can improve outcomes. Most studies have focused on sildenafil (Viagra) which was shown to improve Doppler parameters in animal models and suggested in case series to be effective in increasing human fetal growth velocity.<span><sup>301, 302</sup></span> A small RCT of sildenafil (50 mg three times daily [TDS]) in women with early onset pre-eclampsia reported a prolongation of pregnancy by 4 days, although only 60% of participants had recorded SGA and there was no effect of treatment on birthweight.<span><sup>303</sup></span> However, prospective RCTs focusing on FGR have failed to show any benefit. Results from the international STRIDER collaboration did not show any prolongation in pregnancy or improvement in outcome from sildenafil (25 mg TDS) treatment.<span><sup>304, 305</sup></span> The Dutch arm of STRIDER study was stopped early because of safety concerns, although meta-analysis of outcomes from the three studies has failed to show a conclusively detrimental effect.<span><sup>306</sup></span> Tadalafil, a longer acting PDE5 inhibitor has also been tested in case reports with reported improved neonatal outcome and no adverse effects, but no RCT evidence is currently available.<span><sup>307, 308</sup></span> Therefore although some studies have suggested benefit using PDE5 inhibitors to improve outcomes in FGR pregnancies, the negative results from STRIDER do not support the use of these drugs outside of clinical trials for the treatment or prevention of FGR. <i>[Evidence level 1+]</i></p><p>RCT evidence does not support the use of LMWH as an effective treatment to prevent SGA or FGR, even in the presence of heritable thrombophilia, and should only be used in women at risk of thromboembolic disease.<span><sup>157, 158, 160, 161</sup></span> There is insufficient evidence that administration of LMWH to pregnancies with FGR prolongs or improves pregnancy outcome.<span><sup>309</sup></span> <i>[Evidence level 1++]</i></p><p>The birth of a preterm, or early term newborn, based on concerns regarding fetal growth should be optimised. Caring for women and babies at the time of an extremely premature birth is challenging. Detailed guidance is provided by the British Association of Perinatal Medicine (BAPM).<span><sup>354</sup></span> This section refers to recommendations for perinatal optimisation when active care is planned for the birth of a baby with FGR. The care of babies at 22<sup>+0</sup>–23<sup>+6</sup> weeks of gestation is particularly challenging and parents must be supported by personalised counselling to help them decide how they wish their baby to be cared for as detailed in the BAPM framework.</p><p>\\n \\n </p><p>As discussed in section 4, the birth of a baby with FGR is a major risk factor for FGR in a subsequent pregnancy and the postnatal period offers an opportunity to address modifiable risk factors. The most important of these is reducing exposure to second-hand smoke. NICE guideline [NG209] recommends that maternity services establish links with contraceptive services, fertility clinics and antenatal and postnatal services so that everyone working in those organisations knows about local stop-smoking support. This will reduce the risk of newborn babies being exposed to second-hand smoke and reduce the number of women going into their next pregnancy as a smoker.<span><sup>83</sup></span></p><p>Following the birth of a baby with FGR, investigations should be offered to try to determine the underlying cause and help provide an opportunity to discuss risk of recurrence and possible interventions to reduce risk at a prepregnancy appointment. These investigations should consider placental histopathology which may be useful<span><sup>372</sup></span> (as recommended by the Royal College of Pathologists defined as birthweight below the 10<sup>th</sup> centile with an abnormal fetal growth curve) and investigation for acquired thrombophilias.<span><sup>373</sup></span> <i>[Evidence level 2–]</i></p><p>Modifiable risk factors should be addressed such as lifestyle factors (e.g. smoking, BMI) and medical conditions optimised. Plans for prevention (i.e. aspirin) and monitoring in future pregnancies should be discussed.</p><p>None.</p><p>All those involved in the development of the Green-top Guidelines, including the Guidelines Committee, Guidelines Committee co-chairs, guideline developers, peer reviewers and other reviewers, are unpaid volunteers and receive no direct funding for their work in producing the guideline. The exception to this are the RCOG staff involved who are salaried employees of the College and Guidelines Committee members who receive reimbursement for expenses for attending Guidelines Committee meetings. Please see more information on travel expense rules on the RCOG website.</p><p>RKM is the chair of the RCOG Scientific Advisory Committee, Deputy National Specialty Lead for Reproductive Health and Childbirth Clinical Research Network NIHR and President of the British Maternal Fetal Medicine Society. EJ received a NERC RESPIRE grant. CL is chief investigator of the TRUFFLE 2 study of moderate preterm fetal growth restriction and has received NIHR HTA funding to Imperial College London. VM has declared no conflicts of interest. GS has received the following funding, paid to their institution: contract from Wellcome Leap for maternal serum proteomics to understand and to predict pregnancy complications leading to stillbirth, contract from Roche Diagnostics Ltd. For an Investigator Initiated Study Agreement: Pregnancy Outcome Prediction Study 2; grants from MRC for pre-labour invasion of the human uterus by Streptococcus agalactiae, from the Wellcome Trust for the evaluation and development of novel diagnostic methods to understand and prevent placentally-related complications of human pregnancy, from the NIHR Cambridge Biomedical Research Centre as Theme Leader for Women's Health and Paediatrics and from the MRC for a quantitative serum metabolite ratio to predict fetal growth abnormalities. They have also personally received a consulting fee from GSK as consultant and member of expert panel for RSV vaccination in pregnancy.</p><p>None.</p>\",\"PeriodicalId\":50729,\"journal\":{\"name\":\"Bjog-An International Journal of Obstetrics and Gynaecology\",\"volume\":\"131 9\",\"pages\":\"e31-e80\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-05-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1471-0528.17814\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bjog-An International Journal of Obstetrics and Gynaecology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://obgyn.onlinelibrary.wiley.com/doi/10.1111/1471-0528.17814\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bjog-An International Journal of Obstetrics and Gynaecology","FirstCategoryId":"3","ListUrlMain":"https://obgyn.onlinelibrary.wiley.com/doi/10.1111/1471-0528.17814","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Investigation and Care of a Small-for-Gestational-Age Fetus and a Growth Restricted Fetus (Green-top Guideline No. 31)
The purpose of this guideline is to provide advice, based on the best evidence available, to guide clinicians regarding the investigation and care of the small-for-gestational-age (SGA) fetus and growth restricted fetus. The guideline reviews the risk factors for these conditions and provides recommendations regarding surveillance, diagnosis, and management, including recommendations for fetal monitoring and birth. Large for gestational age (LGA) is outside the scope of this guidance.
This guideline is for healthcare professionals who care for women, non-binary and trans people with a SGA fetus or with fetal growth restriction (FGR). Within this document we use the terms woman and women's health. However, it is important to acknowledge that it is not only women for whom it is necessary to access women's health and reproductive services in order to maintain their gynaecological health and reproductive wellbeing. Gynaecological and obstetric services and delivery of care must therefore be appropriate, inclusive and sensitive to the needs of those individuals whose gender identity does not align with the sex they were assigned at birth.
Fetal size is measured at a single time point in pregnancy and assessed via individual biometric measurements (e.g. head circumference [HC], abdominal circumference [AC], and femur length [FL]) or measurements combined as estimated fetal weight (EFW) using different formulas. Fetal growth is a dynamic process occurring throughout the pregnancy requiring multiple assessments and a minimum of at least two assessments of fetal size. Additional information that can be considered includes maternal history and symptoms, amniotic fluid assessment and Doppler velocimetry. Any measurement obtained (biometry or EFW) can only be interpreted when plotted on a growth chart to determine both the centile of the measurement but also any change in growth trajectory. Growth charts are discussed further in section 7.2.1.
An appropriate for gestational age (AGA) fetus is one whose size is within a normal range for its gestational age. This is typically defined as between the 10th and 90th centiles. A fetus is considered SGA when individual biometric measurements or a combination of measurements used to estimate fetal weight fall below set parameters and requires accurate assessment of gestational age. Commonly, the definition of SGA refers to a fetus with a predicted weight or an AC measurement less than the 10th centile. SGA at birth is commonly diagnosed based on a birthweight below the 10th centile and often birthweight charts are adjusted for the sex of the baby.
FGR implies a pathological restriction of the genetic growth potential.1, 2 Some, but not all, growth restricted fetuses/infants are SGA. The likelihood of FGR is higher in fetuses that are smaller.3 Growth restricted fetuses may manifest evidence of fetal compromise (abnormal Doppler studies, reduced liquor volume).
Defining FGR and thus diagnosing it in a current pregnancy is challenging because of the need to determine growth potential. Similarly, risk assessing whether FGR existed in a previous pregnancy presents a different challenge. There is a need to focus on those fetuses at risk of adverse outcome and thus those that are FGR rather than SGA using varying parameters such as sequential ultrasound measurements, Doppler assessments, and biomarkers. FGR can also be subdivided clinically into early and late depending on the gestational age, with variation in gestational thresholds between 32 and 37 weeks.
A Delphi consensus-based definition of FGR (Table 1) has been suggested for use both in clinical practice and in research for early (defined in the Delphi consensus as before 32+0 weeks) and late onset FGR.4, 5
Saving Babies Lives Care Bundle version 3 (SBLCBv3) suggests practical definitions for FGR in a previous pregnancy, FGR in the current pregnancy, and suboptimal growth.6 It highlights that absent or reversed end diastolic flow in the umbilical artery is a feature of early onset FGR, but importantly that absence of this feature (for example, a normal umbilical artery Doppler) from 32+0 weeks of gestation does not mean that the fetus is not growth restricted and does not rule out the possibility of fetal compromise.
Suboptimal fetal growth may also be indicative of FGR and can be diagnosed when a previously well-grown fetus (i.e. size 10th centile or above) fails to maintain adequate fetal growth during pregnancy. Suboptimal growth is difficult to define, with SBLCBv3 defining it as a pattern of slowing growth velocity (i.e. a downward trend in the centile).6 The Delphi consensus defines it as AC/EFW crossing centiles greater than two quartiles on non-customised growth centiles ≥32+0 weeks (equivalent to 50 centiles).5 Static growth can be defined as no forward growth velocity in EFW, or AC measured at least 14 days apart. Suboptimal fetal growth is further addressed in section 7.3.2.
Low birthweight (LBW) refers to an infant with a birthweight less than 2500 g regardless of gestation. This is no longer used in clinical practice as the majority of pregnancies have an early dating scan therefore birthweight can be adjusted for gestational age. This definition is included for interpretation of older research papers only. FGR has previously been described as symmetrical or asymmetrical and it has been proposed that it may help determine possible aetiology. However, this feature can vary and is not prognostic of outcome8 so should no longer be used as a description of FGR.
Small fetuses are divided into normal (constitutionally small), non-placenta mediated growth restriction (e.g. structural, or chromosomal anomaly, inborn errors of metabolism and fetal infection), and placenta mediated growth restriction (placental dysfunction). Maternal factors such as low pre-pregnancy weight, undernutrition, substance misuse or severe anaemia can affect placental transfer of nutrients. Medical conditions can also affect placental implantation and vasculature and hence transfer (pre-eclampsia, autoimmune disease, thrombophilias, renal disease, diabetes, cardiac disease, and essential hypertension).
The underlying aetiology as well as timing of onset is important when considering the risk of adverse outcome in pregnancy. Early onset FGR is associated with significant and abnormal placentation that results in increased hypoxia and cardiovascular adaptions9 and therefore carries an increased risk of adverse perinatal mortality and morbidity.10 Early FGR also often coexists with maternal manifestations of placental dysfunction (hypertensive disorders of pregnancy) or maternal medical conditions and thus is easier to detect through screening pathways. In late onset FGR, the deficit in placentation is milder, with less cardiovascular adaption and a lower risk of adverse events. However, late FGR is more common, and it is more difficult to identify fetuses that may be at risk (on ultrasound scan [USS]) and thus detect, and therefore these pregnancies account for a significant proportion of adverse outcomes. They are, therefore, an important area for effective surveillance and management.
Serial symphysis fundal height (SFH) measurement is a method of surveillance for fetal size, however, it has a low sensitivity for detecting SGA/FGR fetuses.11 Suspicion of a fetal growth disorder usually relies on ultrasound measurement of fetal AC or estimation of fetal weight. Care of the SGA/FGR fetus is directed at timely birth. Several surveillance tests are available, including cardiotocography (CTG), Doppler and USS to assess biophysical activity, but there is controversy about which test or combination of tests should be used to time birth in late onset FGR and SGA.
The NHS England SBLCB (a care bundle for reducing perinatal mortality) was first published in 2016 and focussed on detection and management of SGA (rather than FGR) and recommended birth at 37+0 to 37+6 weeks for SGA, as did the 2013 version of this RCOG guidance.12 The SpiRE evaluation of the SBLCB version 1 demonstrated a measurable difference in antenatal detection of SGA babies across England.13 The evaluation also demonstrated an increase in USS and inductions of labour at early term (37+0–38+6 weeks). Thus, by seeking to capture all babies at risk, interventions increased in women who were only marginally at increased risk of FGR-related stillbirth, with risks to the babies of early term induction (namely increased risk of admission to the neonatal unit and potential long-term adverse effects, e.g. increased risk of special educational needs).14, 15 This was partly addressed in version 2 of the bundle (2019), with different management strategies for SGA and FGR to try and reduce unnecessary intervention in SGA babies not at risk of adverse outcome.16 SBLCBv3, and this guideline, addresses this further with a focus on detecting FGR and targeting intervention (i.e. birth) for those at increased risk of perinatal death.6
The Cochrane Library and electronic databases (DARE, EMBASE, Trip, MEDLINE and PubMed) were searched using the relevant Medical Subject Headings (MeSH) terms, including all subheadings and synonyms, and this was combined with a keyword search and was limited to humans and English language; search terms included ‘fetal growth retardation’, ‘fetal growth restriction’ and ‘infant, small for gestational age’. The search was restricted to articles published from 2011 until December 2022. The full search strategy is available to view online as supporting information (Appendix S1 and S2). Papers identified by peer reviewers and the developers which fall outside the literature searches and may be more recent have also been included in the evidence base for the guideline.
This guideline was developed using the standard methodology for Green-top Guidelines.17 Where possible, recommendations are based on available evidence. In the absence of published evidence, these have been annotated as ‘good practice points’. Further information about the assessment of evidence and the grading of recommendations may be found in Appendix I.
Risk assessment is a fundamental part of care in the maternity pathway and should be a dynamic process with continual assessment throughout the pregnancy. Risk assessment must always consider previous medical history, obstetric history and current pregnancy history with information obtained from the woman, review of medical notes and contact with previous care providers as necessary.18 All pregnant women should have a risk assessment for FGR carried out by 14 weeks of gestation using an agreed pathway.6
The likelihood of a FGR or FGR-related stillbirth occurring in a pregnancy is influenced by many factors. When considering risk assessment, the following are important: a priori risk (this is the probability of an event occurring that the woman has as she enters the pregnancy based on previous history); absence of risk factors (e.g. if a certain risk factor is not present does this reduce the risk overall and the influence of other risk factors that are present); if multiple risk factors are present how do these interplay and change the level of risk. This information is not known in sufficient detail for many conditions in pregnancy nor related to risk factors for FGR.
Risk assessment in FGR is also challenged by the fact that many analyses of risk factors for fetal growth disorders identify newborns with a birthweight less than the 10th centile as a proxy for FGR, with the majority of these births occurring at term and thus including a significant proportion of heathy smaller babies. Hence, studies using SGA as a proxy for FGR may underestimate the risk of adverse outcomes associated with FGR. This makes evidence assimilation difficult to identify which women should have increased surveillance.
There have been several risk assessment models designed for the prediction of pre-eclampsia that have been used for SGA prediction. There are data from the ASPRE randomised controlled trial (RCT; model for prediction of pre-eclampsia and aspirin administration) and SPREE study (prediction of pre-eclampsia) related to SGA prediction that identifies a high proportion of cases of preterm SGA that can be prevented by the prophylactic use of aspirin.19 As these models are designed for pre-eclampsia prediction, they can be expected to have utility in prediction of FGR associated with placental dysfunction and pre-eclampsia but cannot assess all risk factors for FGR. These are discussed further in section 5.2.4.
Tools used to assess risk should provide a structured, consistent approach that can adapt throughout the pregnancy and support the pregnant woman and her clinician in making decisions about her care by making personalised care recommendations using clinically validated machine learning algorithms. Checklists for the presence of risk factors cannot weigh or assess this interaction between risk factors as described above, they also address risk as a binary function of present or absent and cannot consider all the information available from the presence and “level” of the risk. They also do not provide information in a way that can support decision making. Thus, it is imperative that future research addresses development of prediction models that are designed specifically for FGR and importantly FGR with adverse outcome, so that they can be incorporated into tools such as the Tommy's App,20 a clinical decision tool being developed by Tommy's and the RCOG and other electronic patient record systems.
Within this section, the known risk factors for FGR and relevant evidence are discussed. A pathway for assessing risk and subsequent management is shown in Appendix II. It is recognised that this pathway has some of the limitations of the checklist approach as discussed above. However, this pathway attempts to incorporate all the risk factors detailed below for FGR and provide an assessment of level of risk in keeping with the National Institute for Health and Care Excellence (NICE) guideline [CG62] for pathways of care.18 It is recognised that maternity providers may wish to use technology platforms and validated prediction models for pre-eclampsia and placental dysfunction prediction. Where this is the case, providers must ensure that risk assessment for other FGR risks not related to pre-eclampsia can be facilitated.
Women must also be assessed at booking for conditions where SFH measurements are not appropriate (e.g. raised body mass index [BMI] of 35 kg/m2 or above at booking; presence of fibroids in uterus [based on clinical judgement]).
The risks of a pregnant woman developing early or late onset FGR are strongly linked to concurrent pregnancy risk factors. As a result of this, the prevalence of FGR varies dramatically in different pregnant populations directly influencing the performance of prediction and detection methods. Early onset FGR is a relatively uncommon condition (~0.3%) with late onset FGR being more common.
Historically, identification of severe SGA (either EFW below the 3rd or 5th centile) was used as a marker for aneuploidy and studies which predated widespread population based screening for aneuploidy reported aneuploidy rates of up to 20%.286-288 These data are less applicable in modern practice, because of the widespread use of population-based screening for aneuploidy. However, invasive testing should be considered in the context of severe SGA because of the possibility of other chromosomal abnormalities which can be detected using DNA microarrays. A systematic review and meta-analysis demonstrated that in fetuses undergoing invasive testing for FGR with no other structural anomalies there was a 4% incremental yield of chromosomal microarray analysis (CMA) over karyotyping and a 10% incremental yield in FGR with associated fetal malformations.289[Evidence level 2++]
Prenatal exome sequencing has limited incremental yield over standard karyotyping and microarray in fetuses with isolated FGR. [Evidence 2++]
A large population-based study from Israel reported a 3% detection rate of pathological abnormalities using microarray in the context of FGR, and only a single case out of 13 was an aneuploidy, underlining the transformative effect of population screening for aneuploidy on this association.290 Therefore, when invasive testing is undertaken in the context of SGA fetal biometry, analysis of specimens should include CMA for the detection of microdeletions and microinsertions. In early onset FGR CMA demonstrated an incremental yield over karyotyping of 4.8% in isolated FGR, 10% in FGR with non-structural anomalies and 10.5% in FGR with structural anomalies.291[Evidence level 2+]
A retrospective cohort study reported the associations with a below the 5th centile FL at the time of a 17–22-week anomaly scan (with or without other features).292 The positive likelihood ratio for trisomy 21 was 8.8, for 13/18 it was 6.5 and for other unbalanced structural chromosomal abnormalities it was 17.4, with an absolute risk of 1 in 339. There was an approximate four-fold subsequent risk of both PTB and birth of an SGA infant. This has been confirmed in a systematic review, which demonstrated that an isolated short FL is significantly associated with SGA (OR 4.04, 95% CI 3.63–4.50) and PTB (OR 3.09, 95% CI 1.57–6.08).293[Evidence level 2++]
A case series of 158 fetuses with an AC of the 5th centile or below during a detailed scan at 18–24 weeks (isolated feature) demonstrated two cases of trisomy 21 and a single case of an unbalanced structural chromosomal abnormality (detected by SNP array).294[Evidence level 2–]
Hence, invasive diagnostic testing (amniocentesis, fetal blood sampling or placental biopsy/chorionic villus sampling) should be offered in severely SGA fetuses with structural anomalies and considered in non-anomalous fetuses detected before 23 weeks of gestation, especially if uterine artery Doppler is normal.
Follow-up scans should also be arranged given the association with subsequent birth of an SGA infant and the timing of commencement and frequency individualised following the additional investigations.
Fetal infections are responsible for up to 5% of SGA fetuses.295 The most common pathogens are reported to be cytomegalovirus (CMV), toxoplasmosis, malaria and syphilis, although a multicentre study found no association between congenital toxoplasmosis and incidence of a SGA infant.295, 296 A full maternal TORCH screen is unnecessary and testing should be based on history and presentation.297 Malaria is a significant cause of PTB and LBW worldwide and it should be considered in those from, or who have travelled in, endemic areas.298 In congenital Zika virus infection, FGR is seen in 10% of affected pregnancies, and a femur-sparing pattern of FGR is commonly seen.299[Evidence level 2–]
There are no proven interventions in SGA and FGR other than birth of the baby. Experimental treatments under investigation in early phase clinical trials/studies include maternal VEGF (vascular endothelial growth factor) gene therapy, melatonin and for pre-eclampsia with the potential to impact on fetal growth; statins, nitric oxide donors, proton pump inhibitors and N-acetycysteine. Preclinical investigations are underway in nanoparticles, microRNAs, hydrogen sulphide and creatinine.300
PDE5 inhibitors have been tested in women with early onset placental disease, including FGR pregnancies to determine if they can improve outcomes. Most studies have focused on sildenafil (Viagra) which was shown to improve Doppler parameters in animal models and suggested in case series to be effective in increasing human fetal growth velocity.301, 302 A small RCT of sildenafil (50 mg three times daily [TDS]) in women with early onset pre-eclampsia reported a prolongation of pregnancy by 4 days, although only 60% of participants had recorded SGA and there was no effect of treatment on birthweight.303 However, prospective RCTs focusing on FGR have failed to show any benefit. Results from the international STRIDER collaboration did not show any prolongation in pregnancy or improvement in outcome from sildenafil (25 mg TDS) treatment.304, 305 The Dutch arm of STRIDER study was stopped early because of safety concerns, although meta-analysis of outcomes from the three studies has failed to show a conclusively detrimental effect.306 Tadalafil, a longer acting PDE5 inhibitor has also been tested in case reports with reported improved neonatal outcome and no adverse effects, but no RCT evidence is currently available.307, 308 Therefore although some studies have suggested benefit using PDE5 inhibitors to improve outcomes in FGR pregnancies, the negative results from STRIDER do not support the use of these drugs outside of clinical trials for the treatment or prevention of FGR. [Evidence level 1+]
RCT evidence does not support the use of LMWH as an effective treatment to prevent SGA or FGR, even in the presence of heritable thrombophilia, and should only be used in women at risk of thromboembolic disease.157, 158, 160, 161 There is insufficient evidence that administration of LMWH to pregnancies with FGR prolongs or improves pregnancy outcome.309[Evidence level 1++]
The birth of a preterm, or early term newborn, based on concerns regarding fetal growth should be optimised. Caring for women and babies at the time of an extremely premature birth is challenging. Detailed guidance is provided by the British Association of Perinatal Medicine (BAPM).354 This section refers to recommendations for perinatal optimisation when active care is planned for the birth of a baby with FGR. The care of babies at 22+0–23+6 weeks of gestation is particularly challenging and parents must be supported by personalised counselling to help them decide how they wish their baby to be cared for as detailed in the BAPM framework.
As discussed in section 4, the birth of a baby with FGR is a major risk factor for FGR in a subsequent pregnancy and the postnatal period offers an opportunity to address modifiable risk factors. The most important of these is reducing exposure to second-hand smoke. NICE guideline [NG209] recommends that maternity services establish links with contraceptive services, fertility clinics and antenatal and postnatal services so that everyone working in those organisations knows about local stop-smoking support. This will reduce the risk of newborn babies being exposed to second-hand smoke and reduce the number of women going into their next pregnancy as a smoker.83
Following the birth of a baby with FGR, investigations should be offered to try to determine the underlying cause and help provide an opportunity to discuss risk of recurrence and possible interventions to reduce risk at a prepregnancy appointment. These investigations should consider placental histopathology which may be useful372 (as recommended by the Royal College of Pathologists defined as birthweight below the 10th centile with an abnormal fetal growth curve) and investigation for acquired thrombophilias.373[Evidence level 2–]
Modifiable risk factors should be addressed such as lifestyle factors (e.g. smoking, BMI) and medical conditions optimised. Plans for prevention (i.e. aspirin) and monitoring in future pregnancies should be discussed.
None.
All those involved in the development of the Green-top Guidelines, including the Guidelines Committee, Guidelines Committee co-chairs, guideline developers, peer reviewers and other reviewers, are unpaid volunteers and receive no direct funding for their work in producing the guideline. The exception to this are the RCOG staff involved who are salaried employees of the College and Guidelines Committee members who receive reimbursement for expenses for attending Guidelines Committee meetings. Please see more information on travel expense rules on the RCOG website.
RKM is the chair of the RCOG Scientific Advisory Committee, Deputy National Specialty Lead for Reproductive Health and Childbirth Clinical Research Network NIHR and President of the British Maternal Fetal Medicine Society. EJ received a NERC RESPIRE grant. CL is chief investigator of the TRUFFLE 2 study of moderate preterm fetal growth restriction and has received NIHR HTA funding to Imperial College London. VM has declared no conflicts of interest. GS has received the following funding, paid to their institution: contract from Wellcome Leap for maternal serum proteomics to understand and to predict pregnancy complications leading to stillbirth, contract from Roche Diagnostics Ltd. For an Investigator Initiated Study Agreement: Pregnancy Outcome Prediction Study 2; grants from MRC for pre-labour invasion of the human uterus by Streptococcus agalactiae, from the Wellcome Trust for the evaluation and development of novel diagnostic methods to understand and prevent placentally-related complications of human pregnancy, from the NIHR Cambridge Biomedical Research Centre as Theme Leader for Women's Health and Paediatrics and from the MRC for a quantitative serum metabolite ratio to predict fetal growth abnormalities. They have also personally received a consulting fee from GSK as consultant and member of expert panel for RSV vaccination in pregnancy.
期刊介绍:
BJOG is an editorially independent publication owned by the Royal College of Obstetricians and Gynaecologists (RCOG). The Journal publishes original, peer-reviewed work in all areas of obstetrics and gynaecology, including contraception, urogynaecology, fertility, oncology and clinical practice. Its aim is to publish the highest quality medical research in women''s health, worldwide.

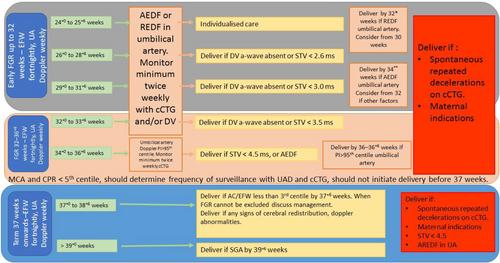

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


