{"title":"用最少的药物和睡眠调节对长期混合状态进行长期管理。","authors":"Verinder Sharma, Katelyn N. Wood","doi":"10.1111/bdi.13454","DOIUrl":null,"url":null,"abstract":"<p>A 72-year-old married nurse was referred to our clinic 16 years ago for the management of treatment-resistant bipolar II disorder. The illness began after the birth of her first child when she was 27 years old. She had a recurrence of depression after the birth of her other two children. Each postpartum episode lasted 4–6 weeks and remitted spontaneously. She first sought professional help when she was 45, and the following year was hospitalized for depression for the first time. In 8 years, she required 13 hospital admissions (see Figure 1), including one hospitalization after an intentional drug overdose. She spent a total of 382 days with hospitalizations ranging in duration between 3 and 83 days. She had to quit her job due to the persistent and disabling nature of the disorder. Following her last hospitalization, her mood continued to fluctuate between periods of mixed depression and hypomania without intervening euthymic intervals. Due to rapid shifts in her moods, she was also thought to have borderline personality disorder and histrionic traits. Her family history was positive for bipolar disorder in at least nine members across three generations including her grandfather, grandmother, aunts, mother, brother, and daughter. Several family members had been treated with lithium and some had received electroconvulsive therapy.</p><p>Past efforts to treat the mood disorder involved trials of antidepressants including amitriptyline, fluvoxamine, nefazodone, moclobemide, and desipramine; lithium, carbamazepine, valproic acid, aripiprazole, paliperidone, methylphenidate, and benzodiazepines. Pindolol was used to augment some of the antidepressants. She developed tachyphylaxis to some of the antidepressants while others were ineffective. She had both unilateral and bilateral electroconvulsive therapy (a total of 19 treatments) that led to confusion and made her more anxious and agitated. Except for amitriptyline, the doses of antidepressants were either adequate or high (e.g., fluvoxamine 400 mg daily). She developed neutropenia requiring discontinuation of carbamazepine; valproate was ineffective, and there was no response to two trials of lithium in combination with antidepressants. She had individual psychotherapy and dialectical behavior therapy without benefit. In terms of her physical health, she had fibromyalgia, migraine, hyperthyroidism (treated with radioactive iodine), and hypertension.</p><p>At the time of her referral to our program, she was taking topiramate 50 mg, bupropion XL 450 mg, gabapentin 2800 mg, and zopiclone 15 mg a day. Aided by collateral information from her family, the diagnosis of bipolar II disorder was confirmed using the DSM-IV. Since the unmedicated illness was marked by episodes of “pure” depression with full inter-episodic recovery, we surmised that the continuous use of antidepressants (alone or in combination with other psychotropic drugs) over the previous 15 years had likely contributed to a perpetual mixed state and treatment refractoriness. During this time, the prominent symptoms were intense anxiety, agitation, irritability, argumentativeness, severe insomnia, and dysphoria. In close collaboration with the patient, we developed a treatment plan to clarify the illness course as follows: (1) taper off and discontinue topiramate, gabapentin, and bupropion, one medication at a time, (2) close monitoring of changes in mood and sleep, and (3) add quetiapine in a low dose to promote sleep. She noted the “clearing” of her thoughts, especially after the discontinuation of topiramate and gabapentin. The zopiclone dose was reduced to 7.5 mg daily.</p><p>Over time, it became clear that she had a hypomania–depression–euthymic interval illness course, and sleep loss/insomnia was an early symptom of impending hypomania. Over the last 16 years, the quetiapine dose has fluctuated between 75 and 125 mg daily. She titrates the dose to manage anticipated hypo/manic or mixed episodes by regulating sleep. She has had brief mood episodes that have remitted following the optimization of the quetiapine dose. She had one jet lag-triggered hypomanic episode that required the addition of olanzapine for a couple of weeks. In anticipation of the heightened risk of recurrence of hypo/mania after a surgical procedure requiring general anesthesia, she was prescribed olanzapine. Notably, immediately after the operation, she developed hyperactive delirium that resolved quickly following a short trial of olanzapine. She has not required a psychiatric hospitalization in 22 years and has been functioning well. She attends her appointments every 3–4 months and actively participates in psychoeducational sessions. She gave written informed consent after reviewing the contents of this report.</p><p>It took more than 25 years for our patient to receive the diagnosis of bipolar disorder despite clear red flags including the first onset of depression after childbirth, a strong family history of bipolar disorder, loss of response to antidepressants,<span><sup>1</sup></span> treatment refractoriness, and hypomanic/mixed episodes. Before treatment-seeking, the depressive episodes were marked by symptoms typically associated with bipolar depression including hypersomnia, psychomotor retardation, and acute onset and offset. As the illness progressed, a failure to specifically elicit information about hypomania may have contributed to the delay in receiving the correct diagnosis. Systemic issues also preclude a diagnosis of bipolar II disorder due to the requirement of confirmation of hypomania among individuals with major depression. The sole emphasis on hypomania ignores other important hallmarks of bipolar disorder including an early age at illness onset, periodicity, poor response to antidepressants, and family history of bipolar disorder. Moreover, the use of neuroleptics and/or benzodiazepine may have prevented or attenuated the expression of hypomania.</p><p>The variability and shifting of symptoms make it difficult to detect mixed symptoms and contribute to the labeling of these symptoms as manifestations of a personality disorder. Our decision to stop the antidepressant and avoid these medications was useful for two reasons. First, it clarified the illness course as it was no longer modified by the chronic administration of antidepressants.<span><sup>2</sup></span> Second, it may have reduced the need for polypharmacy due to the improvement in her sleep, anxiety, and agitation following the discontinuation of antidepressants. There is a paucity of data on the maintenance treatment of bipolar mixed states. Suggested options include quetiapine alone or in combination with other medications, lithium, and olanzapine.<span><sup>3</sup></span> The quetiapine dose used in this case was lower than the dose normally indicated for bipolar depression (300–600 mg daily), suggesting that the low dose to manage insomnia, or decreased sleep requirement as a symptom of hypomania was effective in preventing depression.</p><p>Initially proposed by Koukopoulos, the primacy of mania hypothesis does not consider mania and depression as opposites but rather interconnected entities suggesting that treatment of hypo/mania might prevent the ensuing depression. Sleep loss due to a reduced need for sleep or resulting from insomnia is common in individuals with bipolar disorder. Females with bipolar disorder appear to be particularly susceptible to sleep loss. Due to the bidirectional relationship between sleep and mood,<span><sup>4</sup></span> the sleep loss likely perpetuated and worsened the mood symptoms in our patient.</p><p>In summary, we describe the successful treatment of a female with bipolar II disorder who, after failing to respond to various pharmacological and psychotherapeutic modalities, experienced a sustained improvement in her mood and functioning following the discontinuation of antidepressants<span><sup>4</sup></span> and a trial of quetiapine and zopiclone in low doses. A personalized approach<span><sup>5</sup></span> specifically targeting sleep loss resulting from a decreased need for sleep or related to external events was effective in the prevention of hypomanic/mixed episodes and consequent depression.</p><p>We declare no competing interests.</p><p>The individual on whom this paper is written consented to participate in the research and has reviewed and approved this manuscript for publication.</p>","PeriodicalId":8959,"journal":{"name":"Bipolar Disorders","volume":"26 7","pages":"750-752"},"PeriodicalIF":5.0000,"publicationDate":"2024-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bdi.13454","citationCount":"0","resultStr":"{\"title\":\"Long-term management of a perpetual mixed state with minimal medication and sleep regulation\",\"authors\":\"Verinder Sharma, Katelyn N. Wood\",\"doi\":\"10.1111/bdi.13454\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 72-year-old married nurse was referred to our clinic 16 years ago for the management of treatment-resistant bipolar II disorder. The illness began after the birth of her first child when she was 27 years old. She had a recurrence of depression after the birth of her other two children. Each postpartum episode lasted 4–6 weeks and remitted spontaneously. She first sought professional help when she was 45, and the following year was hospitalized for depression for the first time. In 8 years, she required 13 hospital admissions (see Figure 1), including one hospitalization after an intentional drug overdose. She spent a total of 382 days with hospitalizations ranging in duration between 3 and 83 days. She had to quit her job due to the persistent and disabling nature of the disorder. Following her last hospitalization, her mood continued to fluctuate between periods of mixed depression and hypomania without intervening euthymic intervals. Due to rapid shifts in her moods, she was also thought to have borderline personality disorder and histrionic traits. Her family history was positive for bipolar disorder in at least nine members across three generations including her grandfather, grandmother, aunts, mother, brother, and daughter. Several family members had been treated with lithium and some had received electroconvulsive therapy.</p><p>Past efforts to treat the mood disorder involved trials of antidepressants including amitriptyline, fluvoxamine, nefazodone, moclobemide, and desipramine; lithium, carbamazepine, valproic acid, aripiprazole, paliperidone, methylphenidate, and benzodiazepines. Pindolol was used to augment some of the antidepressants. She developed tachyphylaxis to some of the antidepressants while others were ineffective. She had both unilateral and bilateral electroconvulsive therapy (a total of 19 treatments) that led to confusion and made her more anxious and agitated. Except for amitriptyline, the doses of antidepressants were either adequate or high (e.g., fluvoxamine 400 mg daily). She developed neutropenia requiring discontinuation of carbamazepine; valproate was ineffective, and there was no response to two trials of lithium in combination with antidepressants. She had individual psychotherapy and dialectical behavior therapy without benefit. In terms of her physical health, she had fibromyalgia, migraine, hyperthyroidism (treated with radioactive iodine), and hypertension.</p><p>At the time of her referral to our program, she was taking topiramate 50 mg, bupropion XL 450 mg, gabapentin 2800 mg, and zopiclone 15 mg a day. Aided by collateral information from her family, the diagnosis of bipolar II disorder was confirmed using the DSM-IV. Since the unmedicated illness was marked by episodes of “pure” depression with full inter-episodic recovery, we surmised that the continuous use of antidepressants (alone or in combination with other psychotropic drugs) over the previous 15 years had likely contributed to a perpetual mixed state and treatment refractoriness. During this time, the prominent symptoms were intense anxiety, agitation, irritability, argumentativeness, severe insomnia, and dysphoria. In close collaboration with the patient, we developed a treatment plan to clarify the illness course as follows: (1) taper off and discontinue topiramate, gabapentin, and bupropion, one medication at a time, (2) close monitoring of changes in mood and sleep, and (3) add quetiapine in a low dose to promote sleep. She noted the “clearing” of her thoughts, especially after the discontinuation of topiramate and gabapentin. The zopiclone dose was reduced to 7.5 mg daily.</p><p>Over time, it became clear that she had a hypomania–depression–euthymic interval illness course, and sleep loss/insomnia was an early symptom of impending hypomania. Over the last 16 years, the quetiapine dose has fluctuated between 75 and 125 mg daily. She titrates the dose to manage anticipated hypo/manic or mixed episodes by regulating sleep. She has had brief mood episodes that have remitted following the optimization of the quetiapine dose. She had one jet lag-triggered hypomanic episode that required the addition of olanzapine for a couple of weeks. In anticipation of the heightened risk of recurrence of hypo/mania after a surgical procedure requiring general anesthesia, she was prescribed olanzapine. Notably, immediately after the operation, she developed hyperactive delirium that resolved quickly following a short trial of olanzapine. She has not required a psychiatric hospitalization in 22 years and has been functioning well. She attends her appointments every 3–4 months and actively participates in psychoeducational sessions. She gave written informed consent after reviewing the contents of this report.</p><p>It took more than 25 years for our patient to receive the diagnosis of bipolar disorder despite clear red flags including the first onset of depression after childbirth, a strong family history of bipolar disorder, loss of response to antidepressants,<span><sup>1</sup></span> treatment refractoriness, and hypomanic/mixed episodes. Before treatment-seeking, the depressive episodes were marked by symptoms typically associated with bipolar depression including hypersomnia, psychomotor retardation, and acute onset and offset. As the illness progressed, a failure to specifically elicit information about hypomania may have contributed to the delay in receiving the correct diagnosis. Systemic issues also preclude a diagnosis of bipolar II disorder due to the requirement of confirmation of hypomania among individuals with major depression. The sole emphasis on hypomania ignores other important hallmarks of bipolar disorder including an early age at illness onset, periodicity, poor response to antidepressants, and family history of bipolar disorder. Moreover, the use of neuroleptics and/or benzodiazepine may have prevented or attenuated the expression of hypomania.</p><p>The variability and shifting of symptoms make it difficult to detect mixed symptoms and contribute to the labeling of these symptoms as manifestations of a personality disorder. Our decision to stop the antidepressant and avoid these medications was useful for two reasons. First, it clarified the illness course as it was no longer modified by the chronic administration of antidepressants.<span><sup>2</sup></span> Second, it may have reduced the need for polypharmacy due to the improvement in her sleep, anxiety, and agitation following the discontinuation of antidepressants. There is a paucity of data on the maintenance treatment of bipolar mixed states. Suggested options include quetiapine alone or in combination with other medications, lithium, and olanzapine.<span><sup>3</sup></span> The quetiapine dose used in this case was lower than the dose normally indicated for bipolar depression (300–600 mg daily), suggesting that the low dose to manage insomnia, or decreased sleep requirement as a symptom of hypomania was effective in preventing depression.</p><p>Initially proposed by Koukopoulos, the primacy of mania hypothesis does not consider mania and depression as opposites but rather interconnected entities suggesting that treatment of hypo/mania might prevent the ensuing depression. Sleep loss due to a reduced need for sleep or resulting from insomnia is common in individuals with bipolar disorder. Females with bipolar disorder appear to be particularly susceptible to sleep loss. Due to the bidirectional relationship between sleep and mood,<span><sup>4</sup></span> the sleep loss likely perpetuated and worsened the mood symptoms in our patient.</p><p>In summary, we describe the successful treatment of a female with bipolar II disorder who, after failing to respond to various pharmacological and psychotherapeutic modalities, experienced a sustained improvement in her mood and functioning following the discontinuation of antidepressants<span><sup>4</sup></span> and a trial of quetiapine and zopiclone in low doses. A personalized approach<span><sup>5</sup></span> specifically targeting sleep loss resulting from a decreased need for sleep or related to external events was effective in the prevention of hypomanic/mixed episodes and consequent depression.</p><p>We declare no competing interests.</p><p>The individual on whom this paper is written consented to participate in the research and has reviewed and approved this manuscript for publication.</p>\",\"PeriodicalId\":8959,\"journal\":{\"name\":\"Bipolar Disorders\",\"volume\":\"26 7\",\"pages\":\"750-752\"},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-05-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bdi.13454\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bipolar Disorders\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/bdi.13454\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bipolar Disorders","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/bdi.13454","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Long-term management of a perpetual mixed state with minimal medication and sleep regulation
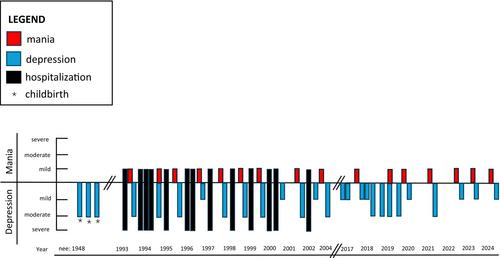
A 72-year-old married nurse was referred to our clinic 16 years ago for the management of treatment-resistant bipolar II disorder. The illness began after the birth of her first child when she was 27 years old. She had a recurrence of depression after the birth of her other two children. Each postpartum episode lasted 4–6 weeks and remitted spontaneously. She first sought professional help when she was 45, and the following year was hospitalized for depression for the first time. In 8 years, she required 13 hospital admissions (see Figure 1), including one hospitalization after an intentional drug overdose. She spent a total of 382 days with hospitalizations ranging in duration between 3 and 83 days. She had to quit her job due to the persistent and disabling nature of the disorder. Following her last hospitalization, her mood continued to fluctuate between periods of mixed depression and hypomania without intervening euthymic intervals. Due to rapid shifts in her moods, she was also thought to have borderline personality disorder and histrionic traits. Her family history was positive for bipolar disorder in at least nine members across three generations including her grandfather, grandmother, aunts, mother, brother, and daughter. Several family members had been treated with lithium and some had received electroconvulsive therapy.
Past efforts to treat the mood disorder involved trials of antidepressants including amitriptyline, fluvoxamine, nefazodone, moclobemide, and desipramine; lithium, carbamazepine, valproic acid, aripiprazole, paliperidone, methylphenidate, and benzodiazepines. Pindolol was used to augment some of the antidepressants. She developed tachyphylaxis to some of the antidepressants while others were ineffective. She had both unilateral and bilateral electroconvulsive therapy (a total of 19 treatments) that led to confusion and made her more anxious and agitated. Except for amitriptyline, the doses of antidepressants were either adequate or high (e.g., fluvoxamine 400 mg daily). She developed neutropenia requiring discontinuation of carbamazepine; valproate was ineffective, and there was no response to two trials of lithium in combination with antidepressants. She had individual psychotherapy and dialectical behavior therapy without benefit. In terms of her physical health, she had fibromyalgia, migraine, hyperthyroidism (treated with radioactive iodine), and hypertension.
At the time of her referral to our program, she was taking topiramate 50 mg, bupropion XL 450 mg, gabapentin 2800 mg, and zopiclone 15 mg a day. Aided by collateral information from her family, the diagnosis of bipolar II disorder was confirmed using the DSM-IV. Since the unmedicated illness was marked by episodes of “pure” depression with full inter-episodic recovery, we surmised that the continuous use of antidepressants (alone or in combination with other psychotropic drugs) over the previous 15 years had likely contributed to a perpetual mixed state and treatment refractoriness. During this time, the prominent symptoms were intense anxiety, agitation, irritability, argumentativeness, severe insomnia, and dysphoria. In close collaboration with the patient, we developed a treatment plan to clarify the illness course as follows: (1) taper off and discontinue topiramate, gabapentin, and bupropion, one medication at a time, (2) close monitoring of changes in mood and sleep, and (3) add quetiapine in a low dose to promote sleep. She noted the “clearing” of her thoughts, especially after the discontinuation of topiramate and gabapentin. The zopiclone dose was reduced to 7.5 mg daily.
Over time, it became clear that she had a hypomania–depression–euthymic interval illness course, and sleep loss/insomnia was an early symptom of impending hypomania. Over the last 16 years, the quetiapine dose has fluctuated between 75 and 125 mg daily. She titrates the dose to manage anticipated hypo/manic or mixed episodes by regulating sleep. She has had brief mood episodes that have remitted following the optimization of the quetiapine dose. She had one jet lag-triggered hypomanic episode that required the addition of olanzapine for a couple of weeks. In anticipation of the heightened risk of recurrence of hypo/mania after a surgical procedure requiring general anesthesia, she was prescribed olanzapine. Notably, immediately after the operation, she developed hyperactive delirium that resolved quickly following a short trial of olanzapine. She has not required a psychiatric hospitalization in 22 years and has been functioning well. She attends her appointments every 3–4 months and actively participates in psychoeducational sessions. She gave written informed consent after reviewing the contents of this report.
It took more than 25 years for our patient to receive the diagnosis of bipolar disorder despite clear red flags including the first onset of depression after childbirth, a strong family history of bipolar disorder, loss of response to antidepressants,1 treatment refractoriness, and hypomanic/mixed episodes. Before treatment-seeking, the depressive episodes were marked by symptoms typically associated with bipolar depression including hypersomnia, psychomotor retardation, and acute onset and offset. As the illness progressed, a failure to specifically elicit information about hypomania may have contributed to the delay in receiving the correct diagnosis. Systemic issues also preclude a diagnosis of bipolar II disorder due to the requirement of confirmation of hypomania among individuals with major depression. The sole emphasis on hypomania ignores other important hallmarks of bipolar disorder including an early age at illness onset, periodicity, poor response to antidepressants, and family history of bipolar disorder. Moreover, the use of neuroleptics and/or benzodiazepine may have prevented or attenuated the expression of hypomania.
The variability and shifting of symptoms make it difficult to detect mixed symptoms and contribute to the labeling of these symptoms as manifestations of a personality disorder. Our decision to stop the antidepressant and avoid these medications was useful for two reasons. First, it clarified the illness course as it was no longer modified by the chronic administration of antidepressants.2 Second, it may have reduced the need for polypharmacy due to the improvement in her sleep, anxiety, and agitation following the discontinuation of antidepressants. There is a paucity of data on the maintenance treatment of bipolar mixed states. Suggested options include quetiapine alone or in combination with other medications, lithium, and olanzapine.3 The quetiapine dose used in this case was lower than the dose normally indicated for bipolar depression (300–600 mg daily), suggesting that the low dose to manage insomnia, or decreased sleep requirement as a symptom of hypomania was effective in preventing depression.
Initially proposed by Koukopoulos, the primacy of mania hypothesis does not consider mania and depression as opposites but rather interconnected entities suggesting that treatment of hypo/mania might prevent the ensuing depression. Sleep loss due to a reduced need for sleep or resulting from insomnia is common in individuals with bipolar disorder. Females with bipolar disorder appear to be particularly susceptible to sleep loss. Due to the bidirectional relationship between sleep and mood,4 the sleep loss likely perpetuated and worsened the mood symptoms in our patient.
In summary, we describe the successful treatment of a female with bipolar II disorder who, after failing to respond to various pharmacological and psychotherapeutic modalities, experienced a sustained improvement in her mood and functioning following the discontinuation of antidepressants4 and a trial of quetiapine and zopiclone in low doses. A personalized approach5 specifically targeting sleep loss resulting from a decreased need for sleep or related to external events was effective in the prevention of hypomanic/mixed episodes and consequent depression.
We declare no competing interests.
The individual on whom this paper is written consented to participate in the research and has reviewed and approved this manuscript for publication.
期刊介绍:
Bipolar Disorders is an international journal that publishes all research of relevance for the basic mechanisms, clinical aspects, or treatment of bipolar disorders and related illnesses. It intends to provide a single international outlet for new research in this area and covers research in the following areas:
biochemistry
physiology
neuropsychopharmacology
neuroanatomy
neuropathology
genetics
brain imaging
epidemiology
phenomenology
clinical aspects
and therapeutics of bipolar disorders
Bipolar Disorders also contains papers that form the development of new therapeutic strategies for these disorders as well as papers on the topics of schizoaffective disorders, and depressive disorders as these can be cyclic disorders with areas of overlap with bipolar disorders.
The journal will consider for publication submissions within the domain of: Perspectives, Research Articles, Correspondence, Clinical Corner, and Reflections. Within these there are a number of types of articles: invited editorials, debates, review articles, original articles, commentaries, letters to the editors, clinical conundrums, clinical curiosities, clinical care, and musings.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


