Carol M E Smyth, Samantha L Winter, John W Dickinson
{"title":"利用光电胸廓成像技术将呼吸模式紊乱与健康呼吸模式区分开来。","authors":"Carol M E Smyth, Samantha L Winter, John W Dickinson","doi":"10.1155/2022/2816781","DOIUrl":null,"url":null,"abstract":"<p><p>There is no gold standard diagnostic method for breathing pattern disorders (BPD) which is commonly diagnosed through the exclusion of other pathologies. Optoelectronic plethysmography (OEP) is a 3D motion capture technique that provides a comprehensive noninvasive assessment of chest wall during rest and exercise. The purpose of this study was to determine if OEP can distinguish between active individuals classified with and without BPD at rest and during exercise. Forty-seven individuals with a healthy breathing pattern (HBP) and twenty-six individuals with a BPD performed a submaximal exercise challenge. OEP measured the movement of the chest wall through the calculation of timing, percentage contribution, and phase angle breathing pattern variables. A mixed model repeated measures ANOVA analysed the OEP variables between the groups classified as HBP and BPD at rest, during exercise, and after recovery. At rest, regional contribution variables including ribcage percentage contribution (HBP: 71% and BPD: 69%), abdominal ribcage contribution (HBP: 13% and BPD: 11%), abdomen percentage contribution (HBP: 29% and BPD: 31%), and ribcage and abdomen volume index (HPB: 2.5 and BPD: 2.2) were significantly (<i>p</i> < 0.05) different between groups. During exercise, BPD displayed significantly (<i>p</i> < 0.05) more asynchrony between various thoracic compartments including the ribcage and abdomen phase angle (HBP: -1.9 and BPD: -2.7), pulmonary ribcage and abdomen phase angle (HBP: -0.5 and BPD, 0.5), abdominal ribcage and shoulders phase angle (HBP: -0.3 and BPD: 0.6), and pulmonary ribcage and shoulders phase angle (HBP: 0.2 and BPD: 0.6). Additionally, the novel variables inhale deviation (HBP: 8.8% and BPD: 19.7%) and exhale deviation (HBP: -10.9% and BPD: -17.6%) were also significantly (<i>p</i> < 0.05) different between the groups during high intensity exercise. Regional contribution and phase angles measured via OEP can distinguish BPD from HBP at rest and during exercise. Characteristics of BPD include asynchronous and thoracic dominant breathing patterns that could form part of future objective criteria for the diagnosis of BPD.</p>","PeriodicalId":75247,"journal":{"name":"Translational sports medicine","volume":"2022 ","pages":"2816781"},"PeriodicalIF":1.9000,"publicationDate":"2022-12-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11022780/pdf/","citationCount":"0","resultStr":"{\"title\":\"Breathing Pattern Disorders Distinguished from Healthy Breathing Patterns Using Optoelectronic Plethysmography.\",\"authors\":\"Carol M E Smyth, Samantha L Winter, John W Dickinson\",\"doi\":\"10.1155/2022/2816781\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>There is no gold standard diagnostic method for breathing pattern disorders (BPD) which is commonly diagnosed through the exclusion of other pathologies. Optoelectronic plethysmography (OEP) is a 3D motion capture technique that provides a comprehensive noninvasive assessment of chest wall during rest and exercise. The purpose of this study was to determine if OEP can distinguish between active individuals classified with and without BPD at rest and during exercise. Forty-seven individuals with a healthy breathing pattern (HBP) and twenty-six individuals with a BPD performed a submaximal exercise challenge. OEP measured the movement of the chest wall through the calculation of timing, percentage contribution, and phase angle breathing pattern variables. A mixed model repeated measures ANOVA analysed the OEP variables between the groups classified as HBP and BPD at rest, during exercise, and after recovery. At rest, regional contribution variables including ribcage percentage contribution (HBP: 71% and BPD: 69%), abdominal ribcage contribution (HBP: 13% and BPD: 11%), abdomen percentage contribution (HBP: 29% and BPD: 31%), and ribcage and abdomen volume index (HPB: 2.5 and BPD: 2.2) were significantly (<i>p</i> < 0.05) different between groups. During exercise, BPD displayed significantly (<i>p</i> < 0.05) more asynchrony between various thoracic compartments including the ribcage and abdomen phase angle (HBP: -1.9 and BPD: -2.7), pulmonary ribcage and abdomen phase angle (HBP: -0.5 and BPD, 0.5), abdominal ribcage and shoulders phase angle (HBP: -0.3 and BPD: 0.6), and pulmonary ribcage and shoulders phase angle (HBP: 0.2 and BPD: 0.6). Additionally, the novel variables inhale deviation (HBP: 8.8% and BPD: 19.7%) and exhale deviation (HBP: -10.9% and BPD: -17.6%) were also significantly (<i>p</i> < 0.05) different between the groups during high intensity exercise. Regional contribution and phase angles measured via OEP can distinguish BPD from HBP at rest and during exercise. Characteristics of BPD include asynchronous and thoracic dominant breathing patterns that could form part of future objective criteria for the diagnosis of BPD.</p>\",\"PeriodicalId\":75247,\"journal\":{\"name\":\"Translational sports medicine\",\"volume\":\"2022 \",\"pages\":\"2816781\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2022-12-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11022780/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational sports medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2022/2816781\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SPORT SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational sports medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/2816781","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SPORT SCIENCES","Score":null,"Total":0}
Breathing Pattern Disorders Distinguished from Healthy Breathing Patterns Using Optoelectronic Plethysmography.
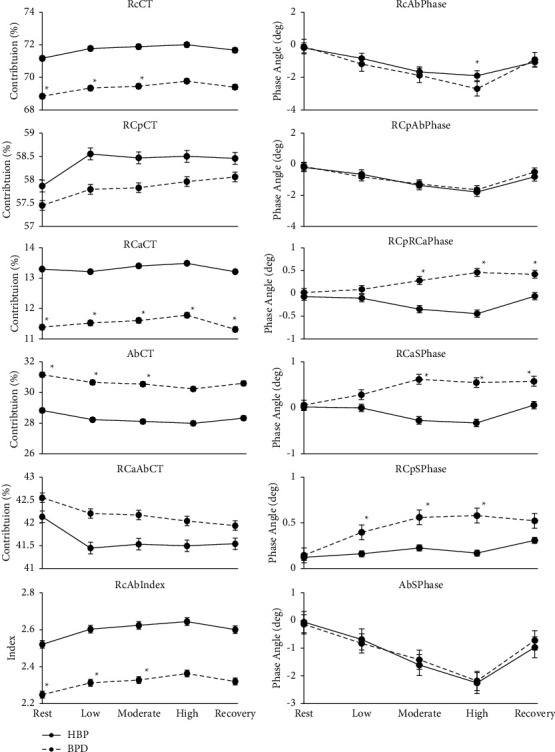
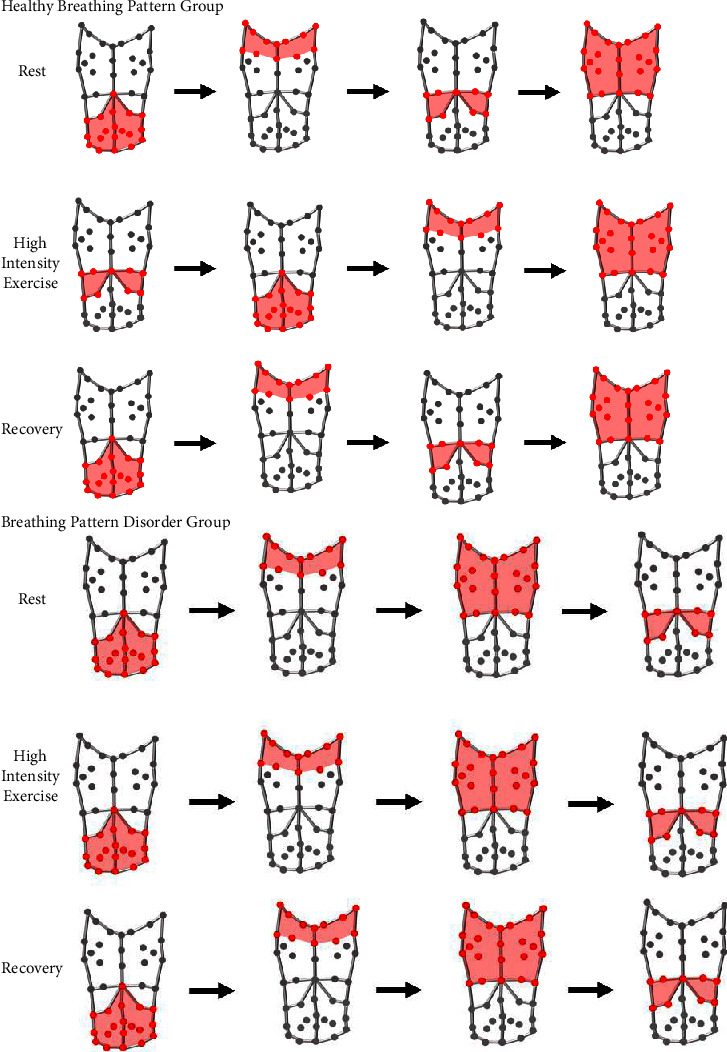
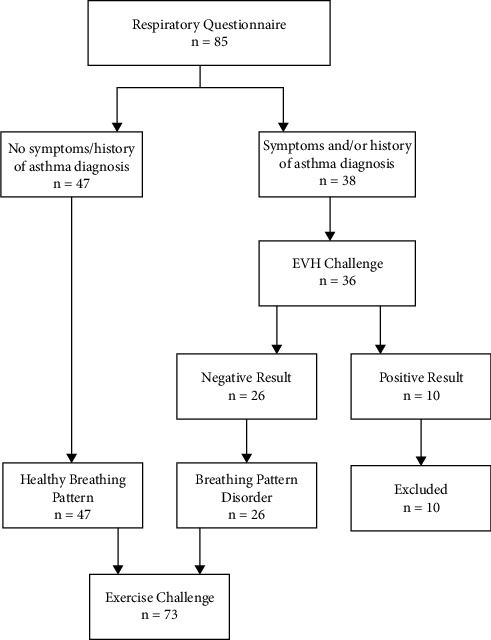
There is no gold standard diagnostic method for breathing pattern disorders (BPD) which is commonly diagnosed through the exclusion of other pathologies. Optoelectronic plethysmography (OEP) is a 3D motion capture technique that provides a comprehensive noninvasive assessment of chest wall during rest and exercise. The purpose of this study was to determine if OEP can distinguish between active individuals classified with and without BPD at rest and during exercise. Forty-seven individuals with a healthy breathing pattern (HBP) and twenty-six individuals with a BPD performed a submaximal exercise challenge. OEP measured the movement of the chest wall through the calculation of timing, percentage contribution, and phase angle breathing pattern variables. A mixed model repeated measures ANOVA analysed the OEP variables between the groups classified as HBP and BPD at rest, during exercise, and after recovery. At rest, regional contribution variables including ribcage percentage contribution (HBP: 71% and BPD: 69%), abdominal ribcage contribution (HBP: 13% and BPD: 11%), abdomen percentage contribution (HBP: 29% and BPD: 31%), and ribcage and abdomen volume index (HPB: 2.5 and BPD: 2.2) were significantly (p < 0.05) different between groups. During exercise, BPD displayed significantly (p < 0.05) more asynchrony between various thoracic compartments including the ribcage and abdomen phase angle (HBP: -1.9 and BPD: -2.7), pulmonary ribcage and abdomen phase angle (HBP: -0.5 and BPD, 0.5), abdominal ribcage and shoulders phase angle (HBP: -0.3 and BPD: 0.6), and pulmonary ribcage and shoulders phase angle (HBP: 0.2 and BPD: 0.6). Additionally, the novel variables inhale deviation (HBP: 8.8% and BPD: 19.7%) and exhale deviation (HBP: -10.9% and BPD: -17.6%) were also significantly (p < 0.05) different between the groups during high intensity exercise. Regional contribution and phase angles measured via OEP can distinguish BPD from HBP at rest and during exercise. Characteristics of BPD include asynchronous and thoracic dominant breathing patterns that could form part of future objective criteria for the diagnosis of BPD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


