{"title":"家族性低脂蛋白血症的当前诊断和管理 1.","authors":"Tetsuji Wakabayashi, Manabu Takahashi, Hiroaki Okazaki, Sachiko Okazaki, Koutaro Yokote, Hayato Tada, Masatsune Ogura, Yasushi Ishigaki, Shizuya Yamashita, Mariko Harada-Shiba","doi":"10.5551/jat.RV22018","DOIUrl":null,"url":null,"abstract":"<p><p>Familial hypobetalipoproteinemia (FHBL) 1 is a rare genetic disorder with an autosomal codominant mode of inheritance and is caused by defects in the apolipoprotein (apo) B (APOB) gene that disable lipoprotein formation. ApoB proteins are required for the formation of very low-density lipoproteins (VLDLs), chylomicrons, and their metabolites. VLDLs transport cholesterol and triglycerides from the liver to the peripheral tissues, whereas chylomicrons transport absorbed lipids and fat-soluble vitamins from the intestine. Homozygous or compound heterozygotes of FHBL1 (HoFHBL1) are extremely rare, and defects in APOB impair VLDL and chylomicron secretion, which result in marked hypolipidemia with malabsorption of fat and fat-soluble vitamins, leading to various complications such as growth disorders, acanthocytosis, retinitis pigmentosa, and neuropathy. Heterozygotes of FHBL1 are relatively common and are generally asymptomatic, except for moderate hypolipidemia and possible hepatic steatosis. If left untreated, HoFHBL1 can cause severe complications and disabilities that are pathologically and phenotypically similar to abetalipoproteinemia (ABL) (an autosomal recessive disorder) caused by mutations in the microsomal triglyceride transfer protein (MTTP) gene. Although HoFHBL1 and ABL cannot be distinguished from the clinical manifestations and laboratory findings of the proband, moderate hypolipidemia in first-degree relatives may help diagnose HoFHBL1. There is currently no specific treatment for HoFHBL1. Palliative therapy including high-dose fat-soluble vitamin supplementation may prevent or delay complications. Registry research on HoFHBL1 is currently ongoing to better understand the disease burden and unmet needs of this life-threatening disease with few therapeutic options.</p>","PeriodicalId":15128,"journal":{"name":"Journal of atherosclerosis and thrombosis","volume":" ","pages":"1005-1023"},"PeriodicalIF":2.8000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11224688/pdf/","citationCount":"0","resultStr":"{\"title\":\"Current Diagnosis and Management of Familial Hypobetalipoproteinemia 1.\",\"authors\":\"Tetsuji Wakabayashi, Manabu Takahashi, Hiroaki Okazaki, Sachiko Okazaki, Koutaro Yokote, Hayato Tada, Masatsune Ogura, Yasushi Ishigaki, Shizuya Yamashita, Mariko Harada-Shiba\",\"doi\":\"10.5551/jat.RV22018\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Familial hypobetalipoproteinemia (FHBL) 1 is a rare genetic disorder with an autosomal codominant mode of inheritance and is caused by defects in the apolipoprotein (apo) B (APOB) gene that disable lipoprotein formation. ApoB proteins are required for the formation of very low-density lipoproteins (VLDLs), chylomicrons, and their metabolites. VLDLs transport cholesterol and triglycerides from the liver to the peripheral tissues, whereas chylomicrons transport absorbed lipids and fat-soluble vitamins from the intestine. Homozygous or compound heterozygotes of FHBL1 (HoFHBL1) are extremely rare, and defects in APOB impair VLDL and chylomicron secretion, which result in marked hypolipidemia with malabsorption of fat and fat-soluble vitamins, leading to various complications such as growth disorders, acanthocytosis, retinitis pigmentosa, and neuropathy. Heterozygotes of FHBL1 are relatively common and are generally asymptomatic, except for moderate hypolipidemia and possible hepatic steatosis. If left untreated, HoFHBL1 can cause severe complications and disabilities that are pathologically and phenotypically similar to abetalipoproteinemia (ABL) (an autosomal recessive disorder) caused by mutations in the microsomal triglyceride transfer protein (MTTP) gene. Although HoFHBL1 and ABL cannot be distinguished from the clinical manifestations and laboratory findings of the proband, moderate hypolipidemia in first-degree relatives may help diagnose HoFHBL1. There is currently no specific treatment for HoFHBL1. Palliative therapy including high-dose fat-soluble vitamin supplementation may prevent or delay complications. Registry research on HoFHBL1 is currently ongoing to better understand the disease burden and unmet needs of this life-threatening disease with few therapeutic options.</p>\",\"PeriodicalId\":15128,\"journal\":{\"name\":\"Journal of atherosclerosis and thrombosis\",\"volume\":\" \",\"pages\":\"1005-1023\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11224688/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of atherosclerosis and thrombosis\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5551/jat.RV22018\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of atherosclerosis and thrombosis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5551/jat.RV22018","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/3 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Current Diagnosis and Management of Familial Hypobetalipoproteinemia 1.
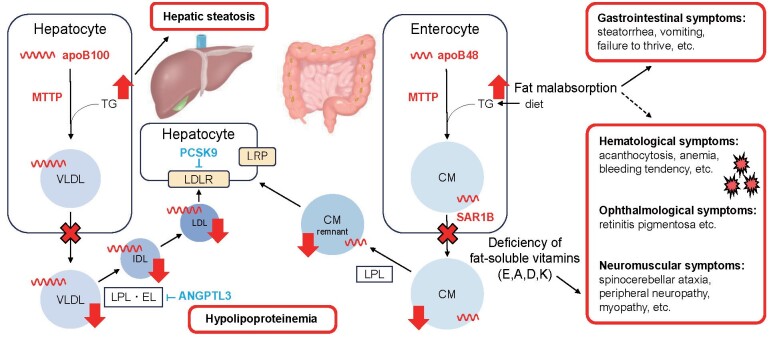
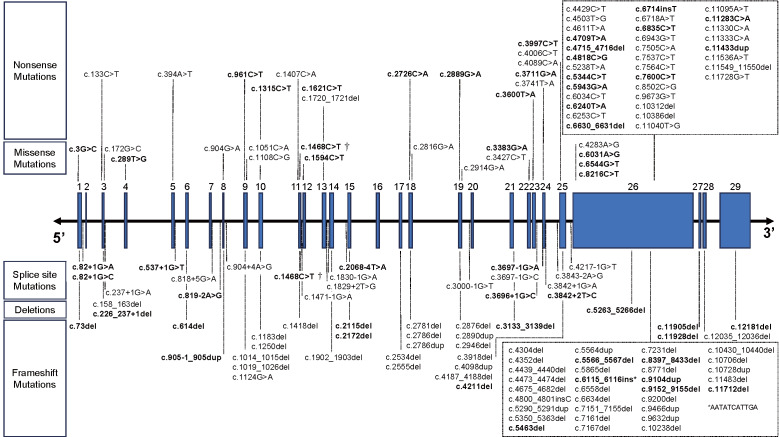
Familial hypobetalipoproteinemia (FHBL) 1 is a rare genetic disorder with an autosomal codominant mode of inheritance and is caused by defects in the apolipoprotein (apo) B (APOB) gene that disable lipoprotein formation. ApoB proteins are required for the formation of very low-density lipoproteins (VLDLs), chylomicrons, and their metabolites. VLDLs transport cholesterol and triglycerides from the liver to the peripheral tissues, whereas chylomicrons transport absorbed lipids and fat-soluble vitamins from the intestine. Homozygous or compound heterozygotes of FHBL1 (HoFHBL1) are extremely rare, and defects in APOB impair VLDL and chylomicron secretion, which result in marked hypolipidemia with malabsorption of fat and fat-soluble vitamins, leading to various complications such as growth disorders, acanthocytosis, retinitis pigmentosa, and neuropathy. Heterozygotes of FHBL1 are relatively common and are generally asymptomatic, except for moderate hypolipidemia and possible hepatic steatosis. If left untreated, HoFHBL1 can cause severe complications and disabilities that are pathologically and phenotypically similar to abetalipoproteinemia (ABL) (an autosomal recessive disorder) caused by mutations in the microsomal triglyceride transfer protein (MTTP) gene. Although HoFHBL1 and ABL cannot be distinguished from the clinical manifestations and laboratory findings of the proband, moderate hypolipidemia in first-degree relatives may help diagnose HoFHBL1. There is currently no specific treatment for HoFHBL1. Palliative therapy including high-dose fat-soluble vitamin supplementation may prevent or delay complications. Registry research on HoFHBL1 is currently ongoing to better understand the disease burden and unmet needs of this life-threatening disease with few therapeutic options.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


