{"title":"与毛囊性真菌病相关的正常脂血黄瘤","authors":"Shunsuke Takahagi MD, PhD, Toshihisa Hamada MD, PhD, Daiki Matsubara MD, PhD","doi":"10.1111/ajd.14300","DOIUrl":null,"url":null,"abstract":"<p>Folliculotropic mycosis fungoides (fMF), a variant of mycosis fungoides, is characterized by infiltration of atypical T cells into the follicular epithelium.<span><sup>1</sup></span> Follicular damage caused by lymphoma cell invasion leads to cyst formation, alopecia and follicular mucinosis. While xanthoma formation within fMF is rare,<span><sup>2, 3</sup></span> its underlying mechanism remains unclear. Additionally, dense histiocytic infiltration may hinder fMF diagnosis.</p><p>A 60-year-old Japanese man presented with a 4-year history of multiple yellowish masses with patchy alopecia on the frontal and parietal scalp (Figure 1a–b). Follicular papules were observed on the trunk and extremities (Figure S1a). Trichoscopy of the patchy alopecia margin showed scaling and crusting at the hair shafts and follicles and milky white structures in the perifollicular region (Figure 1c). In the alopecic area, dilated follicles lacking hair were surrounded by yellowish white structures (Figure 1d). Histologically, a scalp specimen from the alopecia margin revealed mucin deposition and lymphocyte and eosinophil infiltrations within the follicles (Figure 2a–c). The perifollicular region displayed a diffuse infiltration of histiocytes mixed with eosinophils and lymphocytes (Figure 2a, d). In the alopecic area, follicles dilated with keratin plugs had lymphocytic and eosinophilic infiltration (Figure 2e, f). The dermis showed a diffuse and dense infiltration of foamy histiocytes, eosinophils and lymphocytes (Figure 2e, g). The infiltrating lymphocytes showed mild to moderate atypia, CD3 positivity and predominant CD4 over CD8 expression (Figure S1b). Histiocytes exhibited CD68<sup>+</sup> S-100− CD1a− phenotype (Figure 2h). The patient had normal serum lipid levels, sIL-2R 723 U/mL and negative anti-human T-cell lymphotropic virus type 1 antibodies, with no evidence of lymph node or visceral involvement. Despite the obscured lymphomatous features due to dense inflammatory infiltrates with histiocytes, the combination of lymphocytic atypia, clonal T-cell receptor gene rearrangement detected by polymerase chain reaction and characteristic extrascalp skin lesions supported the diagnosis of fMF (stage IIB) with xanthoma. Local radiotherapy, narrow-band ultraviolet B, systemic etretinate and intravenous interferon-gamma helped reduce the scalp masses, leaving xanthoma.</p><p>Kurihara et al.<span><sup>2</sup></span> observed lymphoma regression after treatment, with subsequent xanthoma formation, suggesting that foamy histiocytes aggregate to ingest destroyed tumour cells. In contrast, in the cases reported by Viedma-Martinez et al.<span><sup>3</sup></span> and ours, xanthomatous lesions were present before treatment. In our case, non-lipid-laden histiocytes infiltrated early lesions at the alopecia margin, whereas lipid-laden foamy histiocytes emerged concurrently with follicular destruction in the alopecic area. This implies that the tumour microenvironment first triggers histiocyte infiltration around the follicles. Subsequently, histiocytes may phagocytose lipoproteins released from destroyed follicular units, leading to xanthoma formation.</p><p>Excessive granulomatous/xanthomatous components in fMF may hinder lymphoma diagnosis. Our case displayed a unique clinical presentation of mass formation on the scalp, contrary to previous cases.<span><sup>4</sup></span> Although trichoscopy aids in fMF diagnosis,<span><sup>4</sup></span> its findings vary depending on follicular damage and perifollicular inflammation. In our case, histological analysis revealed dense granulomatous/xanthomatous inflammation, mucin deposition and eosinophilic follicular infiltration, complicating lymphoma cell/lesion identification. A comprehensive assessment involving lymphocytic atypia, genetic clonality, extrascalp lesions and multiple biopsies from different sites may ensure a definitive diagnosis of fMF complicated by those secondary reactions, including dense histiocytic infiltrates.</p><p>Shunsuke Takahagi contributed to analysis and interpretation of data, and was involved in writing the manuscript. Toshihisa Hamada contributed to analysis and interpretation of data, and was involved in writing the manuscript. Daiki Matsubara contributed to collection and analysis of data. All authors read and approved the final manuscript.</p><p>There were no funding sources.</p><p>Authors have no conflicts of interest to declare.</p><p>The patient gave consent for his photographs and medical information to be published in print and online and with the understanding that this information may be publicly available.</p>","PeriodicalId":8638,"journal":{"name":"Australasian Journal of Dermatology","volume":null,"pages":null},"PeriodicalIF":2.2000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ajd.14300","citationCount":"0","resultStr":"{\"title\":\"Normolipemic xanthoma associated with folliculotropic mycosis fungoides\",\"authors\":\"Shunsuke Takahagi MD, PhD, Toshihisa Hamada MD, PhD, Daiki Matsubara MD, PhD\",\"doi\":\"10.1111/ajd.14300\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Folliculotropic mycosis fungoides (fMF), a variant of mycosis fungoides, is characterized by infiltration of atypical T cells into the follicular epithelium.<span><sup>1</sup></span> Follicular damage caused by lymphoma cell invasion leads to cyst formation, alopecia and follicular mucinosis. While xanthoma formation within fMF is rare,<span><sup>2, 3</sup></span> its underlying mechanism remains unclear. Additionally, dense histiocytic infiltration may hinder fMF diagnosis.</p><p>A 60-year-old Japanese man presented with a 4-year history of multiple yellowish masses with patchy alopecia on the frontal and parietal scalp (Figure 1a–b). Follicular papules were observed on the trunk and extremities (Figure S1a). Trichoscopy of the patchy alopecia margin showed scaling and crusting at the hair shafts and follicles and milky white structures in the perifollicular region (Figure 1c). In the alopecic area, dilated follicles lacking hair were surrounded by yellowish white structures (Figure 1d). Histologically, a scalp specimen from the alopecia margin revealed mucin deposition and lymphocyte and eosinophil infiltrations within the follicles (Figure 2a–c). The perifollicular region displayed a diffuse infiltration of histiocytes mixed with eosinophils and lymphocytes (Figure 2a, d). In the alopecic area, follicles dilated with keratin plugs had lymphocytic and eosinophilic infiltration (Figure 2e, f). The dermis showed a diffuse and dense infiltration of foamy histiocytes, eosinophils and lymphocytes (Figure 2e, g). The infiltrating lymphocytes showed mild to moderate atypia, CD3 positivity and predominant CD4 over CD8 expression (Figure S1b). Histiocytes exhibited CD68<sup>+</sup> S-100− CD1a− phenotype (Figure 2h). The patient had normal serum lipid levels, sIL-2R 723 U/mL and negative anti-human T-cell lymphotropic virus type 1 antibodies, with no evidence of lymph node or visceral involvement. Despite the obscured lymphomatous features due to dense inflammatory infiltrates with histiocytes, the combination of lymphocytic atypia, clonal T-cell receptor gene rearrangement detected by polymerase chain reaction and characteristic extrascalp skin lesions supported the diagnosis of fMF (stage IIB) with xanthoma. Local radiotherapy, narrow-band ultraviolet B, systemic etretinate and intravenous interferon-gamma helped reduce the scalp masses, leaving xanthoma.</p><p>Kurihara et al.<span><sup>2</sup></span> observed lymphoma regression after treatment, with subsequent xanthoma formation, suggesting that foamy histiocytes aggregate to ingest destroyed tumour cells. In contrast, in the cases reported by Viedma-Martinez et al.<span><sup>3</sup></span> and ours, xanthomatous lesions were present before treatment. In our case, non-lipid-laden histiocytes infiltrated early lesions at the alopecia margin, whereas lipid-laden foamy histiocytes emerged concurrently with follicular destruction in the alopecic area. This implies that the tumour microenvironment first triggers histiocyte infiltration around the follicles. Subsequently, histiocytes may phagocytose lipoproteins released from destroyed follicular units, leading to xanthoma formation.</p><p>Excessive granulomatous/xanthomatous components in fMF may hinder lymphoma diagnosis. Our case displayed a unique clinical presentation of mass formation on the scalp, contrary to previous cases.<span><sup>4</sup></span> Although trichoscopy aids in fMF diagnosis,<span><sup>4</sup></span> its findings vary depending on follicular damage and perifollicular inflammation. In our case, histological analysis revealed dense granulomatous/xanthomatous inflammation, mucin deposition and eosinophilic follicular infiltration, complicating lymphoma cell/lesion identification. A comprehensive assessment involving lymphocytic atypia, genetic clonality, extrascalp lesions and multiple biopsies from different sites may ensure a definitive diagnosis of fMF complicated by those secondary reactions, including dense histiocytic infiltrates.</p><p>Shunsuke Takahagi contributed to analysis and interpretation of data, and was involved in writing the manuscript. Toshihisa Hamada contributed to analysis and interpretation of data, and was involved in writing the manuscript. Daiki Matsubara contributed to collection and analysis of data. All authors read and approved the final manuscript.</p><p>There were no funding sources.</p><p>Authors have no conflicts of interest to declare.</p><p>The patient gave consent for his photographs and medical information to be published in print and online and with the understanding that this information may be publicly available.</p>\",\"PeriodicalId\":8638,\"journal\":{\"name\":\"Australasian Journal of Dermatology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ajd.14300\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Australasian Journal of Dermatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ajd.14300\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"DERMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Australasian Journal of Dermatology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ajd.14300","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DERMATOLOGY","Score":null,"Total":0}
Normolipemic xanthoma associated with folliculotropic mycosis fungoides
Folliculotropic mycosis fungoides (fMF), a variant of mycosis fungoides, is characterized by infiltration of atypical T cells into the follicular epithelium.1 Follicular damage caused by lymphoma cell invasion leads to cyst formation, alopecia and follicular mucinosis. While xanthoma formation within fMF is rare,2, 3 its underlying mechanism remains unclear. Additionally, dense histiocytic infiltration may hinder fMF diagnosis.
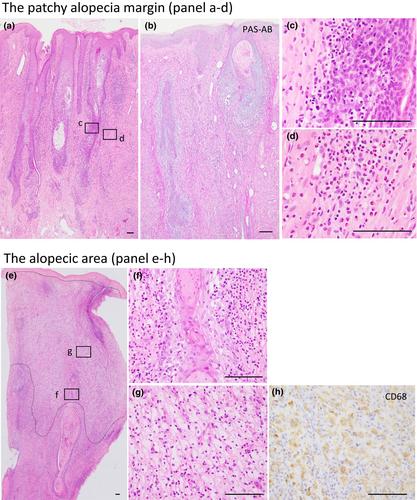
A 60-year-old Japanese man presented with a 4-year history of multiple yellowish masses with patchy alopecia on the frontal and parietal scalp (Figure 1a–b). Follicular papules were observed on the trunk and extremities (Figure S1a). Trichoscopy of the patchy alopecia margin showed scaling and crusting at the hair shafts and follicles and milky white structures in the perifollicular region (Figure 1c). In the alopecic area, dilated follicles lacking hair were surrounded by yellowish white structures (Figure 1d). Histologically, a scalp specimen from the alopecia margin revealed mucin deposition and lymphocyte and eosinophil infiltrations within the follicles (Figure 2a–c). The perifollicular region displayed a diffuse infiltration of histiocytes mixed with eosinophils and lymphocytes (Figure 2a, d). In the alopecic area, follicles dilated with keratin plugs had lymphocytic and eosinophilic infiltration (Figure 2e, f). The dermis showed a diffuse and dense infiltration of foamy histiocytes, eosinophils and lymphocytes (Figure 2e, g). The infiltrating lymphocytes showed mild to moderate atypia, CD3 positivity and predominant CD4 over CD8 expression (Figure S1b). Histiocytes exhibited CD68+ S-100− CD1a− phenotype (Figure 2h). The patient had normal serum lipid levels, sIL-2R 723 U/mL and negative anti-human T-cell lymphotropic virus type 1 antibodies, with no evidence of lymph node or visceral involvement. Despite the obscured lymphomatous features due to dense inflammatory infiltrates with histiocytes, the combination of lymphocytic atypia, clonal T-cell receptor gene rearrangement detected by polymerase chain reaction and characteristic extrascalp skin lesions supported the diagnosis of fMF (stage IIB) with xanthoma. Local radiotherapy, narrow-band ultraviolet B, systemic etretinate and intravenous interferon-gamma helped reduce the scalp masses, leaving xanthoma.
Kurihara et al.2 observed lymphoma regression after treatment, with subsequent xanthoma formation, suggesting that foamy histiocytes aggregate to ingest destroyed tumour cells. In contrast, in the cases reported by Viedma-Martinez et al.3 and ours, xanthomatous lesions were present before treatment. In our case, non-lipid-laden histiocytes infiltrated early lesions at the alopecia margin, whereas lipid-laden foamy histiocytes emerged concurrently with follicular destruction in the alopecic area. This implies that the tumour microenvironment first triggers histiocyte infiltration around the follicles. Subsequently, histiocytes may phagocytose lipoproteins released from destroyed follicular units, leading to xanthoma formation.
Excessive granulomatous/xanthomatous components in fMF may hinder lymphoma diagnosis. Our case displayed a unique clinical presentation of mass formation on the scalp, contrary to previous cases.4 Although trichoscopy aids in fMF diagnosis,4 its findings vary depending on follicular damage and perifollicular inflammation. In our case, histological analysis revealed dense granulomatous/xanthomatous inflammation, mucin deposition and eosinophilic follicular infiltration, complicating lymphoma cell/lesion identification. A comprehensive assessment involving lymphocytic atypia, genetic clonality, extrascalp lesions and multiple biopsies from different sites may ensure a definitive diagnosis of fMF complicated by those secondary reactions, including dense histiocytic infiltrates.
Shunsuke Takahagi contributed to analysis and interpretation of data, and was involved in writing the manuscript. Toshihisa Hamada contributed to analysis and interpretation of data, and was involved in writing the manuscript. Daiki Matsubara contributed to collection and analysis of data. All authors read and approved the final manuscript.
There were no funding sources.
Authors have no conflicts of interest to declare.
The patient gave consent for his photographs and medical information to be published in print and online and with the understanding that this information may be publicly available.
期刊介绍:
Australasian Journal of Dermatology is the official journal of the Australasian College of Dermatologists and the New Zealand Dermatological Society, publishing peer-reviewed, original research articles, reviews and case reports dealing with all aspects of clinical practice and research in dermatology. Clinical presentations, medical and physical therapies and investigations, including dermatopathology and mycology, are covered. Short articles may be published under the headings ‘Signs, Syndromes and Diagnoses’, ‘Dermatopathology Presentation’, ‘Vignettes in Contact Dermatology’, ‘Surgery Corner’ or ‘Letters to the Editor’.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


