Jud C. Janak, Ryan D. Ross, Brenna L. Brady, Liisa Palmer, Jeffrey T. Howard, Joshua F. Baker
{"title":"处方 JAKi 和 TNFi 的类风湿关节炎患者中心血管和癌症风险因素的流行情况:Merative公司的一项MarketScan横断面研究","authors":"Jud C. Janak, Ryan D. Ross, Brenna L. Brady, Liisa Palmer, Jeffrey T. Howard, Joshua F. Baker","doi":"10.1002/acr.25356","DOIUrl":null,"url":null,"abstract":"<div>\n \n <section>\n \n <h3> Objective</h3>\n \n <p>The study was to determine the prevalence of baseline risk factors for cardiovascular outcomes and cancer among commercially-insured patients with rheumatoid arthritis (RA) during their first dispensed treatment for either tumor necrosis factor inhibitors (TNFi) or JAK inhibitors (JAKi).</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Patients with RA from August 16, 2019 to March 31, 2022 were identified in the Merative MarketScan Commercial and Medicare databases. The first date that a TNFi or JAKi was dispensed was the index date, and baseline risk factors were assessed among patients continuously eligible for 12 months before the index date. Patients who had the following were stratified into an elevated risk category: age ≥65 years, smoking, or a history of a major adverse cardiovascular event, venous thromboembolism, or cancer. The prevalence of modifiable risk factors was also reported: hypertension, hyperlipidemia, obesity, and diabetes. The crude prevalence and prevalence difference (PD) were reported.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 12,673 patients (TNFi [n = 7,748; 61%] and JAKi [n = 4,925; 39%]) met inclusion criteria. The prevalence of elevated risk was the same for all patients using TNFi (n = 2,051; 26%) and JAKi (n = 1,262; 26%). Compared with patients having low risk, patients with an elevated risk also had a higher prevalence of at least one primary modifiable risk factor for both patients using JAKi (79% vs 58%; PD 21%, 95% confidence interval [CI] 18%–24%) and TNFi (81% vs 60%; PD 21%, 95% CI 19%–23%).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>In recent years, JAKi and TNFi were used in similar proportions to treat RA among commercially-insured patients at elevated cardiovascular and cancer risk. Because uncontrolled disease, modifiable comorbidities, and treatment with JAKi are associated with these adverse events, future studies evaluating how practice patterns may be affected by the emergence of safety data will be of value.</p>\n </section>\n </div>","PeriodicalId":8406,"journal":{"name":"Arthritis Care & Research","volume":null,"pages":null},"PeriodicalIF":3.7000,"publicationDate":"2024-04-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/acr.25356","citationCount":"0","resultStr":"{\"title\":\"Prevalence of Cardiovascular and Cancer Risk Factors Among Rheumatoid Arthritis Patients Prescribed JAK Inhibitors and Tumor Necrosis Factor Inhibitors: A Cross-Sectional Study\",\"authors\":\"Jud C. Janak, Ryan D. Ross, Brenna L. Brady, Liisa Palmer, Jeffrey T. Howard, Joshua F. Baker\",\"doi\":\"10.1002/acr.25356\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>The study was to determine the prevalence of baseline risk factors for cardiovascular outcomes and cancer among commercially-insured patients with rheumatoid arthritis (RA) during their first dispensed treatment for either tumor necrosis factor inhibitors (TNFi) or JAK inhibitors (JAKi).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Patients with RA from August 16, 2019 to March 31, 2022 were identified in the Merative MarketScan Commercial and Medicare databases. The first date that a TNFi or JAKi was dispensed was the index date, and baseline risk factors were assessed among patients continuously eligible for 12 months before the index date. Patients who had the following were stratified into an elevated risk category: age ≥65 years, smoking, or a history of a major adverse cardiovascular event, venous thromboembolism, or cancer. The prevalence of modifiable risk factors was also reported: hypertension, hyperlipidemia, obesity, and diabetes. The crude prevalence and prevalence difference (PD) were reported.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 12,673 patients (TNFi [n = 7,748; 61%] and JAKi [n = 4,925; 39%]) met inclusion criteria. The prevalence of elevated risk was the same for all patients using TNFi (n = 2,051; 26%) and JAKi (n = 1,262; 26%). Compared with patients having low risk, patients with an elevated risk also had a higher prevalence of at least one primary modifiable risk factor for both patients using JAKi (79% vs 58%; PD 21%, 95% confidence interval [CI] 18%–24%) and TNFi (81% vs 60%; PD 21%, 95% CI 19%–23%).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>In recent years, JAKi and TNFi were used in similar proportions to treat RA among commercially-insured patients at elevated cardiovascular and cancer risk. Because uncontrolled disease, modifiable comorbidities, and treatment with JAKi are associated with these adverse events, future studies evaluating how practice patterns may be affected by the emergence of safety data will be of value.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8406,\"journal\":{\"name\":\"Arthritis Care & Research\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":3.7000,\"publicationDate\":\"2024-04-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/acr.25356\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Arthritis Care & Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/acr.25356\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arthritis Care & Research","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/acr.25356","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目标确定首次接受 TNFi 或 JAKi 治疗的商业保险类风湿性关节炎(RA)患者中心血管疾病和癌症基线风险因素的流行率。方法在 Merative MarketScan® 商业和医疗保险数据库中识别 8/16/2019-3/31/2022 年期间的 RA 患者。以首次配发 TNFi 或 JAKi 为指标日期,对指标前 12 个月内连续符合条件的患者进行基线风险因素评估。患者被分为 "高 "风险类别:年龄≥65 岁、吸烟和/或有重大不良心血管事件 (MACE)、静脉血栓栓塞 (VTE) 或癌症病史。还报告了可改变的风险因素的患病率:高血压、高脂血症、肥胖和糖尿病。结果 共有12,673名患者[TNFi(7,748人;61%)和JAKi(4,925人;39%)]符合纳入标准。所有TNFi(n=2,051;26%)和JAKi(n=1,262;26%)患者的 "高风险 "发生率相同。与低风险患者相比,JAKi [79% vs. 58%; PD: 21% (95%CI: 18%-24%)]和 TNFi [81% vs. 60%; PD: 21% (95%CI: 19%-23%)]患者中风险升高患者的至少一个主要可改变风险因素的发生率也更高。由于未控制的疾病、可改变的并发症以及使用 JAKi 治疗与这些不良事件有关,因此未来对安全性数据的出现如何影响实践模式进行评估的研究将非常有价值。
Prevalence of Cardiovascular and Cancer Risk Factors Among Rheumatoid Arthritis Patients Prescribed JAK Inhibitors and Tumor Necrosis Factor Inhibitors: A Cross-Sectional Study
Objective
The study was to determine the prevalence of baseline risk factors for cardiovascular outcomes and cancer among commercially-insured patients with rheumatoid arthritis (RA) during their first dispensed treatment for either tumor necrosis factor inhibitors (TNFi) or JAK inhibitors (JAKi).
Methods
Patients with RA from August 16, 2019 to March 31, 2022 were identified in the Merative MarketScan Commercial and Medicare databases. The first date that a TNFi or JAKi was dispensed was the index date, and baseline risk factors were assessed among patients continuously eligible for 12 months before the index date. Patients who had the following were stratified into an elevated risk category: age ≥65 years, smoking, or a history of a major adverse cardiovascular event, venous thromboembolism, or cancer. The prevalence of modifiable risk factors was also reported: hypertension, hyperlipidemia, obesity, and diabetes. The crude prevalence and prevalence difference (PD) were reported.
Results
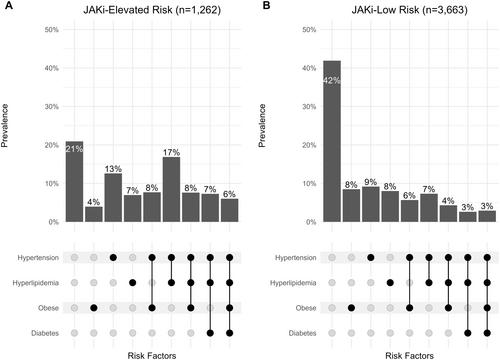
A total of 12,673 patients (TNFi [n = 7,748; 61%] and JAKi [n = 4,925; 39%]) met inclusion criteria. The prevalence of elevated risk was the same for all patients using TNFi (n = 2,051; 26%) and JAKi (n = 1,262; 26%). Compared with patients having low risk, patients with an elevated risk also had a higher prevalence of at least one primary modifiable risk factor for both patients using JAKi (79% vs 58%; PD 21%, 95% confidence interval [CI] 18%–24%) and TNFi (81% vs 60%; PD 21%, 95% CI 19%–23%).
Conclusion
In recent years, JAKi and TNFi were used in similar proportions to treat RA among commercially-insured patients at elevated cardiovascular and cancer risk. Because uncontrolled disease, modifiable comorbidities, and treatment with JAKi are associated with these adverse events, future studies evaluating how practice patterns may be affected by the emergence of safety data will be of value.
期刊介绍:
Arthritis Care & Research, an official journal of the American College of Rheumatology and the Association of Rheumatology Health Professionals (a division of the College), is a peer-reviewed publication that publishes original research, review articles, and editorials that promote excellence in the clinical practice of rheumatology. Relevant to the care of individuals with rheumatic diseases, major topics are evidence-based practice studies, clinical problems, practice guidelines, educational, social, and public health issues, health economics, health care policy, and future trends in rheumatology practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


