{"title":"实施右前或中央切除术时术后胆道并发症与胆道解剖学方面的关系:单中心回顾性观察研究","authors":"Masaki Ueno, Shinya Hayami, Atsushi Miyamoto, Ken-ichi Okada, Yuji Kitahata, Atsushi Shimizu, Hideki Motobayashi, Kyohei Matsumoto, Manabu Kawai","doi":"10.1002/ags3.12805","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>Central liver resections are considered to be high-risk procedures due to postoperative biliary complications. However, anatomical aspect-related causes are underreported. Focusing upon right anterior sectionectomy (H58) and central bisectionectomy (H458), we assessed risk factors for postoperative biliary complications.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We retrospectively reviewed patients who underwent H58 or H458 in our hospital between April 2008 and June 2023 (<i>n</i> = 58). We conducted univariate and multivariate analysis of risk factors of postoperative biliary complications among perioperative factors and anatomical factors including the branching type of the right posterior hepatic duct (RPHD) and the length of the right hepatic duct (RHD).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Twenty-six patients (44.8%) had postoperative biliary complications. Potent risk factors in univariate analysis were the tumor proximity to the right anterior Glissonean branch and longer RHD (both <i>P <</i> 0.01). In multivariate analysis, longer RHD was the only independent risk factor and its hazard (95% confidence interval [CI] was 1.19 (1.05–1.35). Receiver operating characteristics curve (ROC) analysis and the area under the ROC showed that 10 mm was the optimal cutoff value with high discriminatory power (0.72). Considering intraoperative procedures of the right anterior segment Glissonean branch dissection, mass ligation at the second-order branch had marginal risk, especially in patients with RHD >10 mm; its hazard (95% CI) was 5.83 (0.95–35.7).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Anatomical factors of RPHD and RHD influenced postoperative biliary complications in this cohort. The supraportal with RHD type was most common anatomy but considered to be hazardous if the RHD was >10 mm.</p>\n </section>\n </div>","PeriodicalId":8030,"journal":{"name":"Annals of Gastroenterological Surgery","volume":"8 6","pages":"1076-1083"},"PeriodicalIF":2.9000,"publicationDate":"2024-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12805","citationCount":"0","resultStr":"{\"title\":\"Relationship between postoperative biliary complications and biliary anatomical aspects in performing right anterior- or central bisectionectomy: Single-center retrospective observational study\",\"authors\":\"Masaki Ueno, Shinya Hayami, Atsushi Miyamoto, Ken-ichi Okada, Yuji Kitahata, Atsushi Shimizu, Hideki Motobayashi, Kyohei Matsumoto, Manabu Kawai\",\"doi\":\"10.1002/ags3.12805\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aim</h3>\\n \\n <p>Central liver resections are considered to be high-risk procedures due to postoperative biliary complications. However, anatomical aspect-related causes are underreported. Focusing upon right anterior sectionectomy (H58) and central bisectionectomy (H458), we assessed risk factors for postoperative biliary complications.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We retrospectively reviewed patients who underwent H58 or H458 in our hospital between April 2008 and June 2023 (<i>n</i> = 58). We conducted univariate and multivariate analysis of risk factors of postoperative biliary complications among perioperative factors and anatomical factors including the branching type of the right posterior hepatic duct (RPHD) and the length of the right hepatic duct (RHD).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Twenty-six patients (44.8%) had postoperative biliary complications. Potent risk factors in univariate analysis were the tumor proximity to the right anterior Glissonean branch and longer RHD (both <i>P <</i> 0.01). In multivariate analysis, longer RHD was the only independent risk factor and its hazard (95% confidence interval [CI] was 1.19 (1.05–1.35). Receiver operating characteristics curve (ROC) analysis and the area under the ROC showed that 10 mm was the optimal cutoff value with high discriminatory power (0.72). Considering intraoperative procedures of the right anterior segment Glissonean branch dissection, mass ligation at the second-order branch had marginal risk, especially in patients with RHD >10 mm; its hazard (95% CI) was 5.83 (0.95–35.7).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Anatomical factors of RPHD and RHD influenced postoperative biliary complications in this cohort. The supraportal with RHD type was most common anatomy but considered to be hazardous if the RHD was >10 mm.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8030,\"journal\":{\"name\":\"Annals of Gastroenterological Surgery\",\"volume\":\"8 6\",\"pages\":\"1076-1083\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-04-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12805\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterological Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12805\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterological Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12805","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Relationship between postoperative biliary complications and biliary anatomical aspects in performing right anterior- or central bisectionectomy: Single-center retrospective observational study
Aim
Central liver resections are considered to be high-risk procedures due to postoperative biliary complications. However, anatomical aspect-related causes are underreported. Focusing upon right anterior sectionectomy (H58) and central bisectionectomy (H458), we assessed risk factors for postoperative biliary complications.
Methods
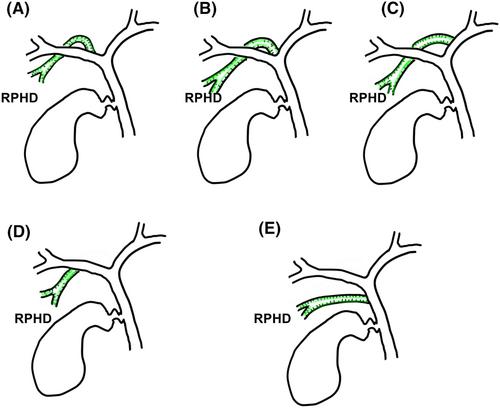
We retrospectively reviewed patients who underwent H58 or H458 in our hospital between April 2008 and June 2023 (n = 58). We conducted univariate and multivariate analysis of risk factors of postoperative biliary complications among perioperative factors and anatomical factors including the branching type of the right posterior hepatic duct (RPHD) and the length of the right hepatic duct (RHD).
Results
Twenty-six patients (44.8%) had postoperative biliary complications. Potent risk factors in univariate analysis were the tumor proximity to the right anterior Glissonean branch and longer RHD (both P < 0.01). In multivariate analysis, longer RHD was the only independent risk factor and its hazard (95% confidence interval [CI] was 1.19 (1.05–1.35). Receiver operating characteristics curve (ROC) analysis and the area under the ROC showed that 10 mm was the optimal cutoff value with high discriminatory power (0.72). Considering intraoperative procedures of the right anterior segment Glissonean branch dissection, mass ligation at the second-order branch had marginal risk, especially in patients with RHD >10 mm; its hazard (95% CI) was 5.83 (0.95–35.7).
Conclusion
Anatomical factors of RPHD and RHD influenced postoperative biliary complications in this cohort. The supraportal with RHD type was most common anatomy but considered to be hazardous if the RHD was >10 mm.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


