Margaret Shyu, Angela Liu, Anya Srikureja, Alison Gregorian, Andrew Srisuwananukorn, Douglas Tremblay, Leonard Naymagon
{"title":"初始直接口服抗凝疗法(DOAC)失败后,使用华法林、达比加群或依诺肝素会有同等的血栓风险","authors":"Margaret Shyu, Angela Liu, Anya Srikureja, Alison Gregorian, Andrew Srisuwananukorn, Douglas Tremblay, Leonard Naymagon","doi":"10.1007/s11239-024-02978-z","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Background</h3><p>The direct oral anticoagulants (DOACs) are now commonly regarded as first line anticoagulants in most cases of venous thromboembolism (VTE). However, the optimal choice of subsequent anticoagulant in instances of first line DOAC failure is unclear.</p><h3 data-test=\"abstract-sub-heading\">Objectives</h3><p>To describe and compare outcomes with second line anticoagulants used after DOAC failure.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>Patients seen at an urban hospital system for an episode of acute VTE initially treated with either apixaban or rivaroxaban who experienced a subsequent recurrent thrombosis while on anticoagulation (1st recurrent thrombosis) were included.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>In total, 166 patients after apixaban or rivaroxaban failure were included. Following DOAC failure (1st recurrent thrombosis), the subsequent anticoagulant was warfarin in 60 patients (36%), dabigatran in 42 patients (25%), and enoxaparin in 64 patients (39%). Enoxaparin was preferentially prescribed in patients with a malignancy-associated etiology for 1st recurrent thrombosis (<i>p</i> < 0.01). The median follow-up time in our cohort was 16 months. There was no difference in 2nd recurrent thrombosis-free survival (<i>p</i> = 0.72) or risk for major bleeding event (<i>p</i> = 0.30) among patients treated with dabigatran, warfarin, or enoxaparin.</p><h3 data-test=\"abstract-sub-heading\">Conclusions</h3><p>In this retrospective analysis of patients failing first line DOAC therapy, rates of 2nd recurrent thrombosis and bleeding did not differ among subsequently chosen anticoagulants. Our study provides evidence that the optimal 2nd anticoagulant is not clear, and the choice of 2nd anticoagulant should continue to balance patient preference, cost, and provider experience.</p>","PeriodicalId":17546,"journal":{"name":"Journal of Thrombosis and Thrombolysis","volume":"211 1","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2024-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Equivalent thrombotic risk with Warfarin, Dabigatran, or Enoxaparin after failure of initial direct oral anticoagulation (DOAC) therapy\",\"authors\":\"Margaret Shyu, Angela Liu, Anya Srikureja, Alison Gregorian, Andrew Srisuwananukorn, Douglas Tremblay, Leonard Naymagon\",\"doi\":\"10.1007/s11239-024-02978-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<h3 data-test=\\\"abstract-sub-heading\\\">Background</h3><p>The direct oral anticoagulants (DOACs) are now commonly regarded as first line anticoagulants in most cases of venous thromboembolism (VTE). However, the optimal choice of subsequent anticoagulant in instances of first line DOAC failure is unclear.</p><h3 data-test=\\\"abstract-sub-heading\\\">Objectives</h3><p>To describe and compare outcomes with second line anticoagulants used after DOAC failure.</p><h3 data-test=\\\"abstract-sub-heading\\\">Methods</h3><p>Patients seen at an urban hospital system for an episode of acute VTE initially treated with either apixaban or rivaroxaban who experienced a subsequent recurrent thrombosis while on anticoagulation (1st recurrent thrombosis) were included.</p><h3 data-test=\\\"abstract-sub-heading\\\">Results</h3><p>In total, 166 patients after apixaban or rivaroxaban failure were included. Following DOAC failure (1st recurrent thrombosis), the subsequent anticoagulant was warfarin in 60 patients (36%), dabigatran in 42 patients (25%), and enoxaparin in 64 patients (39%). Enoxaparin was preferentially prescribed in patients with a malignancy-associated etiology for 1st recurrent thrombosis (<i>p</i> < 0.01). The median follow-up time in our cohort was 16 months. There was no difference in 2nd recurrent thrombosis-free survival (<i>p</i> = 0.72) or risk for major bleeding event (<i>p</i> = 0.30) among patients treated with dabigatran, warfarin, or enoxaparin.</p><h3 data-test=\\\"abstract-sub-heading\\\">Conclusions</h3><p>In this retrospective analysis of patients failing first line DOAC therapy, rates of 2nd recurrent thrombosis and bleeding did not differ among subsequently chosen anticoagulants. Our study provides evidence that the optimal 2nd anticoagulant is not clear, and the choice of 2nd anticoagulant should continue to balance patient preference, cost, and provider experience.</p>\",\"PeriodicalId\":17546,\"journal\":{\"name\":\"Journal of Thrombosis and Thrombolysis\",\"volume\":\"211 1\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-04-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Thrombosis and Thrombolysis\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11239-024-02978-z\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Thrombosis and Thrombolysis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11239-024-02978-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Equivalent thrombotic risk with Warfarin, Dabigatran, or Enoxaparin after failure of initial direct oral anticoagulation (DOAC) therapy
Background
The direct oral anticoagulants (DOACs) are now commonly regarded as first line anticoagulants in most cases of venous thromboembolism (VTE). However, the optimal choice of subsequent anticoagulant in instances of first line DOAC failure is unclear.
Objectives
To describe and compare outcomes with second line anticoagulants used after DOAC failure.
Methods
Patients seen at an urban hospital system for an episode of acute VTE initially treated with either apixaban or rivaroxaban who experienced a subsequent recurrent thrombosis while on anticoagulation (1st recurrent thrombosis) were included.
Results
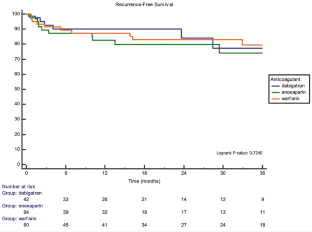
In total, 166 patients after apixaban or rivaroxaban failure were included. Following DOAC failure (1st recurrent thrombosis), the subsequent anticoagulant was warfarin in 60 patients (36%), dabigatran in 42 patients (25%), and enoxaparin in 64 patients (39%). Enoxaparin was preferentially prescribed in patients with a malignancy-associated etiology for 1st recurrent thrombosis (p < 0.01). The median follow-up time in our cohort was 16 months. There was no difference in 2nd recurrent thrombosis-free survival (p = 0.72) or risk for major bleeding event (p = 0.30) among patients treated with dabigatran, warfarin, or enoxaparin.
Conclusions
In this retrospective analysis of patients failing first line DOAC therapy, rates of 2nd recurrent thrombosis and bleeding did not differ among subsequently chosen anticoagulants. Our study provides evidence that the optimal 2nd anticoagulant is not clear, and the choice of 2nd anticoagulant should continue to balance patient preference, cost, and provider experience.
期刊介绍:
The Journal of Thrombosis and Thrombolysis is a long-awaited resource for contemporary cardiologists, hematologists, vascular medicine specialists and clinician-scientists actively involved in treatment decisions and clinical investigation of thrombotic disorders involving the cardiovascular and cerebrovascular systems. The principal focus of the Journal centers on the pathobiology of thrombosis and vascular disorders and the use of anticoagulants, platelet antagonists, cell-based therapies and interventions in scientific investigation, clinical-translational research and patient care.
The Journal will publish original work which emphasizes the interface between fundamental scientific principles and clinical investigation, stimulating an interdisciplinary and scholarly dialogue in thrombosis and vascular science. Published works will also define platforms for translational research, drug development, clinical trials and patient-directed applications. The Journal of Thrombosis and Thrombolysis'' integrated format will expand the reader''s knowledge base and provide important insights for both the investigation and direct clinical application of the most rapidly growing fields in medicine-thrombosis and vascular science.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


