Pierre Gourdy, Patrice Darmon, Isabelle Borget, Corinne Emery, Isabelle Bureau, Bruno Detournay, Amar Bahloul, Noemie Allali, Aymeric Mahieu, Alfred Penfornis
{"title":"法国糖尿病患者的基础胰岛素疗法:EF-BI 研究","authors":"Pierre Gourdy, Patrice Darmon, Isabelle Borget, Corinne Emery, Isabelle Bureau, Bruno Detournay, Amar Bahloul, Noemie Allali, Aymeric Mahieu, Alfred Penfornis","doi":"10.1007/s13300-024-01577-8","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Introduction</h3><p>Second-generation basal insulins like glargine 300 U/mL (Gla-300) have a longer duration of action and less daily fluctuation and interday variability than first-generation ones, such as glargine 100 U/mL (Gla-100). The EF-BI study, a nationwide observational, retrospective study, was designed to compare persistence, acute care complications, and healthcare costs associated with the initiation of such basal insulins (BI) in a real-life setting in France.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>This study was conducted using the French healthcare claims database (SNDS). Adult patients living with type 1 or type 2 diabetes mellitus (T1DM or T2DM) initiating Gla-300 or Gla-100 ± other hypoglycemic medications between January 1, 2016 and December 31, 2020, and without any insulin therapy over the previous 6 months were included. Persistence was defined as remaining on the same insulin therapy until discontinuation defined by a 6 month period without insulin reimbursement. Hospitalized acute complications were identified using ICD-10 codes. Total collective costs were established for patients treated continuously with each basal insulin over 1–3 years. All comparisons were adjusted using a propensity score based on initial patient/treatment characteristics.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>A total of 235,894 patients with T2DM and 6672 patients with T1DM were included. Patients treated with Gla-300 were 83% (T1DM) and 44% (T2DM) less likely to discontinue their treatment than those treated with Gla-100 after 24 months (<i>p</i> < 0.0001). The annual incidence of acute hospitalized events in patients with T2DM treated with Gla-300 was 12% lower than with Gla-100 (<i>p</i> < 0.0001) but similar in patients with T1DM. Comparison of overall costs showed moderate but statistically significant differences in favor of Gla-300 versus Gla-100 for all patients over the first year, and in T2DM only over a 3-year follow-up.</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>Use of Gla-300 resulted in a better persistence, less acute hospitalized events at least in T2DM, and reduced healthcare expenditure. These real-life results confirmed the potential interest of using Gla-300 rather than Gla-100.</p>","PeriodicalId":11192,"journal":{"name":"Diabetes Therapy","volume":"115 1","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2024-04-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Basal Insulinotherapy in Patients Living with Diabetes in France: The EF-BI Study\",\"authors\":\"Pierre Gourdy, Patrice Darmon, Isabelle Borget, Corinne Emery, Isabelle Bureau, Bruno Detournay, Amar Bahloul, Noemie Allali, Aymeric Mahieu, Alfred Penfornis\",\"doi\":\"10.1007/s13300-024-01577-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<h3 data-test=\\\"abstract-sub-heading\\\">Introduction</h3><p>Second-generation basal insulins like glargine 300 U/mL (Gla-300) have a longer duration of action and less daily fluctuation and interday variability than first-generation ones, such as glargine 100 U/mL (Gla-100). The EF-BI study, a nationwide observational, retrospective study, was designed to compare persistence, acute care complications, and healthcare costs associated with the initiation of such basal insulins (BI) in a real-life setting in France.</p><h3 data-test=\\\"abstract-sub-heading\\\">Methods</h3><p>This study was conducted using the French healthcare claims database (SNDS). Adult patients living with type 1 or type 2 diabetes mellitus (T1DM or T2DM) initiating Gla-300 or Gla-100 ± other hypoglycemic medications between January 1, 2016 and December 31, 2020, and without any insulin therapy over the previous 6 months were included. Persistence was defined as remaining on the same insulin therapy until discontinuation defined by a 6 month period without insulin reimbursement. Hospitalized acute complications were identified using ICD-10 codes. Total collective costs were established for patients treated continuously with each basal insulin over 1–3 years. All comparisons were adjusted using a propensity score based on initial patient/treatment characteristics.</p><h3 data-test=\\\"abstract-sub-heading\\\">Results</h3><p>A total of 235,894 patients with T2DM and 6672 patients with T1DM were included. Patients treated with Gla-300 were 83% (T1DM) and 44% (T2DM) less likely to discontinue their treatment than those treated with Gla-100 after 24 months (<i>p</i> < 0.0001). The annual incidence of acute hospitalized events in patients with T2DM treated with Gla-300 was 12% lower than with Gla-100 (<i>p</i> < 0.0001) but similar in patients with T1DM. Comparison of overall costs showed moderate but statistically significant differences in favor of Gla-300 versus Gla-100 for all patients over the first year, and in T2DM only over a 3-year follow-up.</p><h3 data-test=\\\"abstract-sub-heading\\\">Conclusion</h3><p>Use of Gla-300 resulted in a better persistence, less acute hospitalized events at least in T2DM, and reduced healthcare expenditure. These real-life results confirmed the potential interest of using Gla-300 rather than Gla-100.</p>\",\"PeriodicalId\":11192,\"journal\":{\"name\":\"Diabetes Therapy\",\"volume\":\"115 1\",\"pages\":\"\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2024-04-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diabetes Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s13300-024-01577-8\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s13300-024-01577-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Basal Insulinotherapy in Patients Living with Diabetes in France: The EF-BI Study
Introduction
Second-generation basal insulins like glargine 300 U/mL (Gla-300) have a longer duration of action and less daily fluctuation and interday variability than first-generation ones, such as glargine 100 U/mL (Gla-100). The EF-BI study, a nationwide observational, retrospective study, was designed to compare persistence, acute care complications, and healthcare costs associated with the initiation of such basal insulins (BI) in a real-life setting in France.
Methods
This study was conducted using the French healthcare claims database (SNDS). Adult patients living with type 1 or type 2 diabetes mellitus (T1DM or T2DM) initiating Gla-300 or Gla-100 ± other hypoglycemic medications between January 1, 2016 and December 31, 2020, and without any insulin therapy over the previous 6 months were included. Persistence was defined as remaining on the same insulin therapy until discontinuation defined by a 6 month period without insulin reimbursement. Hospitalized acute complications were identified using ICD-10 codes. Total collective costs were established for patients treated continuously with each basal insulin over 1–3 years. All comparisons were adjusted using a propensity score based on initial patient/treatment characteristics.
Results
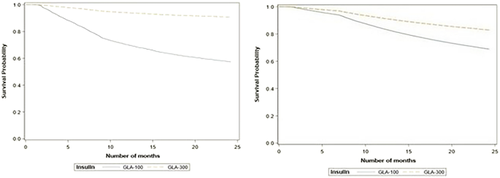
A total of 235,894 patients with T2DM and 6672 patients with T1DM were included. Patients treated with Gla-300 were 83% (T1DM) and 44% (T2DM) less likely to discontinue their treatment than those treated with Gla-100 after 24 months (p < 0.0001). The annual incidence of acute hospitalized events in patients with T2DM treated with Gla-300 was 12% lower than with Gla-100 (p < 0.0001) but similar in patients with T1DM. Comparison of overall costs showed moderate but statistically significant differences in favor of Gla-300 versus Gla-100 for all patients over the first year, and in T2DM only over a 3-year follow-up.
Conclusion
Use of Gla-300 resulted in a better persistence, less acute hospitalized events at least in T2DM, and reduced healthcare expenditure. These real-life results confirmed the potential interest of using Gla-300 rather than Gla-100.
期刊介绍:
Diabetes Therapy is an international, peer reviewed, rapid-publication (peer review in 2 weeks, published 3–4 weeks from acceptance) journal dedicated to the publication of high-quality clinical (all phases), observational, real-world, and health outcomes research around the discovery, development, and use of therapeutics and interventions (including devices) across all areas of diabetes. Studies relating to diagnostics and diagnosis, pharmacoeconomics, public health, epidemiology, quality of life, and patient care, management, and education are also encouraged.
The journal is of interest to a broad audience of healthcare professionals and publishes original research, reviews, communications and letters. The journal is read by a global audience and receives submissions from all over the world. Diabetes Therapy will consider all scientifically sound research be it positive, confirmatory or negative data. Submissions are welcomed whether they relate to an international and/or a country-specific audience, something that is crucially important when researchers are trying to target more specific patient populations. This inclusive approach allows the journal to assist in the dissemination of all scientifically and ethically sound research.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


