Anna Gustafsson, Emma Jonasson, Anders Ståhlberg, Göran Landberg
{"title":"无细胞乳腺癌支架的蛋白质组学鉴定临床相关的印迹蛋白和癌症进展特性","authors":"Anna Gustafsson, Emma Jonasson, Anders Ståhlberg, Göran Landberg","doi":"10.1002/cac2.12542","DOIUrl":null,"url":null,"abstract":"<p>The composition of the extracellular tumor microenvironment (TME) has not been fully delineated, limiting the understanding of general cancer-progressing properties within the cancer niche. The interplay and dynamics between cancer cells and the surrounding structures and cells clearly differ between various subtypes of cancer, adding to the complexity of precision medicine [<span>1</span>].</p><p>To better understand the composition and to define the imprinted proteins of the TME in breast cancer and its potential associations with clinical properties of the disease, we performed global proteomic analysis on a cohort of 63 decellularized patient-derived scaffolds (PDSs). PDSs represents the cell-free TME and were prepared using primary lesions from breast cancer patients with available clinicopathological data (Figure 1A, Supplementary file of methods). The PDS method has earlier been shown to maintain tumor tissue heterogeniety in vitro, producing quantitative assessments of the activity of the TME when studying cancer cell lines adapted to various PDS-based cell cultures [<span>2</span>]. Specific gene changes in the cancer population induced by the heterogenous PDS culture conditions have also been linked to clinical observations, validating the selected strategy for this study [<span>2-5</span>].</p><p>The analysis of the cell-free PDSs identified 1,844 unique proteins (Supplementary Table S1), showing enrichment for proteins related to metabolism, translation, transport, immunity, and extracellular matrix (ECM). Surprisingly, most proteins were annotated as cytoplasmic, suggesting that intracellular proteins were also associated with the PDSs, as further deliberated below (Supplementary Figure S1). When comparing the protein contents from primary cancer samples with adjacent normal breast tissues, 1,280 of the 1,844 detected proteins from the cell-free compartments were differentially expressed. Normal breast tissues were, in comparison to the PDSs, enriched for proteins involved in oxidation-reducing processes, secretion, regulation of exocytosis, and ECM organization (Supplementary Figure S2).</p><p>Next, we used k-means clustering to identify potential subgroups of patients based on the protein composition of the cell-free PDSs. PDS Clusters 1-3 were recognized, distinguished by the expression of proteins in Clusters A-C. Interestingly, the PDS clusters were significantly associated with cancer subtypes (Figure 1B and Supplementary Table S2). Cluster 1 was mainly derived from lobular cancers (63%) and low-grade cancers, showing high levels of 458 proteins involved in ECM organization, biological adhesion, and leukocyte-mediated immunity forming protein Cluster A. Cluster 2 was primarily derived from ductal cancers (77%) and showed pronounced expression of protein Cluster B, comprising of 396 proteins related to exocytosis, secretion and neutrophil degranulation. Cluster 3 included a mixture of ductal and lobular cancers with the highest levels of proteins from Cluster C, containing 990 proteins mainly involved in metabolic processes and establishment of cellular localization. When identifying proteins separating the two cancer types independently of the defined clusters (Figure 1C and Supplementary Table S3), ductal cancers were enriched for proteins classified as modifying enzymes, metabolite interconversion enzymes, RNA metabolism proteins and translational proteins. In contrast, lobular cancers showed high protein contents of ECM and defense/immunity proteins (Figure 1D), supporting earlier findings that subsets of lobular cancers might be more responsive to immune-targeting cancer therapies [<span>1</span>].</p><p>Next, we identified PDS-associated proteins that significantly differed between patients with or without recurrent disease (Figure 1E). The 52 proteins associated with progressive disease and recurrences were mainly classified as transporter and metabolite interconversion enzymes, while the 31 proteins linked to non-recurrent cancer primarily were cytoskeletal and scaffold/adaptor proteins. Interestingly, members of the keratin protein and solute carrier (SLC) families were prominent among the proteins associated with aggressive disease, and 8 out of 14 identified keratins were more abundant in PDSs from patients later having disease recurrences (Figure 1F). Higher levels of KRT78 in PDSs were significantly associated with poor disease-free survival in univariate (Figure 1G) as well as multivariable analyses (hazard ratio = 14.86, <i>P</i> = 0.01). In line with the presented data, keratins are abundantly expressed in subsets of epithelial cells and are linked to prognosis in many cancer types [<span>6</span>].</p><p>To further define the scaffold content in breast cancer, we clustered the PDSs based on a subset of 126 ECM-related proteins traditionally being representative of the TME (Figure 1H and Supplementary Table S4). Three new ECM-based PDS clusters were observed, only partly overlapping with the previous reported clusters (Supplementary Figure S3), and further significantly associated with cancer grade and age of the patients (Supplementary Tables S5-S6). Cluster ECM-1 showed a high proportion of low-grade cancers, mixed patient ages and was distinguished by high presence of collagens, microfibril-associated proteins (EMILIN1, MFAP2), fibrillins (FBN1, FBN2), latent transforming growth factor beta binding protein LTBP1, and peroxidin PRDX4, as well as low levels of integrin subunit ITGB2. Cluster ECM-2 was associated with high-grade cancer, older patient ages and was strongly associated with lower levels of ECM proteins, specifically collagens and laminin subunits, as well as of the structural protein tenascin XB (TNXB). In contrast, cluster ECM-3 mainly included low-grade cancers of all ages and was defined by higher ECM protein content. When detailing the collagen abundance in the PDSs in relation to patient age, there was a significant gradual decrease in 10 out of 21 detected collagens with increasing patient age (Figure 1I).</p><p>Proteins identified in the TME could be important when designing future in vitro three-dimensional (3D) growth models but could also be further evaluated as potential diagnostic biomarkers or even targets for cancer therapies. Importantly, the presented data demonstrate that ECM-related proteins were often more abundant in less malignant low-grade TME. This suggest that 3D growth models mimicking aggressive breast cancer cannot be recapitulated using only ECM proteins but should be complemented with other proteins present in the cancer niche. The age of the cancer patient was also associated with the ECM composition of the PDS, and younger patients exhibited higher level of ECM proteins, specifically collagens. The collagen turnover is a normal part of tissue homeostasis, and collagens commonly becomes more loose, disorganized, and fragmented in older tissues, including the skin [<span>7</span>]. Elderly patients also have different pharmacokinetic profiles compared to younger patients. Based on the obvious structural differences now also demonstrated in the TME, age-specific cancer drugs could be developed and tailored for managing varying malignant properties within the TME of younger or older cancer patients. Regarding the presence of intracellular proteins in the cell-free PDSs from breast cancer patients, other studies exploring ECM proteins in decellularized tissues [<span>8, 9</span>] also detected large amounts of intracellular proteins despite using harsh detergent treatments and enrichment processes. These results support that the multitude of proteins detected in this study indeed represents structurally incorporated and scaffold-associated proteins revealed by the PDS method. The results further suggest that different cell types within the TME are contributing to the imprinting of the scaffold structures, but future studies should detail the potential contribution from secreted and circulating factors.</p><p>In conclusion, the results suggest that breast cancers can be subclassified based on the levels of specific proteins in the cell-free PDS microenvironment. The PDS compositions were not only limited to ECM-associated proteins but also incorporated proteins linked to processes such as secretion, transport, localization, immune response, and metabolism. Importantly, properties of the PDSs were indeed linked to clinical characteristics of the cancer disease, suggesting that different qualities of the TME have the potential to add clinically relevant information for breast cancer.</p><p>A.S and G.L are shareholders and board members of iScaff Pharma AB. The approach using patient-derived scaffolds is patent pending (WO 2018/083231 A1). A.S is shareholder and board member of SiMSen Diagnostics and Tulebovaasta.</p><p>This work was supported by grants from The Swedish Research Council (2019-01273 and 2021-01008), Sweden's Innovation Agency (2017-03737), and Swedish Cancer Foundation (22-2214 and 22-2080), the Swedish state under the agreement between the Swedish government and county councils, the ALF-agreement (965065 and 965580) and BioCARE National Strategic Research Program at University of Gothenburg, Region Västra Götaland, The Sjöberg Foundation, Assar Gabrielssons Research Foundation, Stiftelsen Sigurd och Elsa Goljes Minne, and Kungliga och Hvitfeldtska Stiftelsen.</p><p>Patient consent to process patient material and data was waived for usage of biobanked materials by the Regional Ethics (Region Väst etiknämnd) Committee in Gothenburg, Seweden, while written consent was obtained from all patients donating fresh tissues (DNR: 515-12 and T972-18). Biobank samples were collected from 1980 to 1999 in Sweden, and patients were monitored until November 15, 2012. The study was performed in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines.</p>","PeriodicalId":9495,"journal":{"name":"Cancer Communications","volume":"44 6","pages":"695-699"},"PeriodicalIF":20.1000,"publicationDate":"2024-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12542","citationCount":"0","resultStr":"{\"title\":\"Proteomics of cell-free breast cancer scaffolds identify clinically relevant imprinted proteins and cancer-progressing properties\",\"authors\":\"Anna Gustafsson, Emma Jonasson, Anders Ståhlberg, Göran Landberg\",\"doi\":\"10.1002/cac2.12542\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The composition of the extracellular tumor microenvironment (TME) has not been fully delineated, limiting the understanding of general cancer-progressing properties within the cancer niche. The interplay and dynamics between cancer cells and the surrounding structures and cells clearly differ between various subtypes of cancer, adding to the complexity of precision medicine [<span>1</span>].</p><p>To better understand the composition and to define the imprinted proteins of the TME in breast cancer and its potential associations with clinical properties of the disease, we performed global proteomic analysis on a cohort of 63 decellularized patient-derived scaffolds (PDSs). PDSs represents the cell-free TME and were prepared using primary lesions from breast cancer patients with available clinicopathological data (Figure 1A, Supplementary file of methods). The PDS method has earlier been shown to maintain tumor tissue heterogeniety in vitro, producing quantitative assessments of the activity of the TME when studying cancer cell lines adapted to various PDS-based cell cultures [<span>2</span>]. Specific gene changes in the cancer population induced by the heterogenous PDS culture conditions have also been linked to clinical observations, validating the selected strategy for this study [<span>2-5</span>].</p><p>The analysis of the cell-free PDSs identified 1,844 unique proteins (Supplementary Table S1), showing enrichment for proteins related to metabolism, translation, transport, immunity, and extracellular matrix (ECM). Surprisingly, most proteins were annotated as cytoplasmic, suggesting that intracellular proteins were also associated with the PDSs, as further deliberated below (Supplementary Figure S1). When comparing the protein contents from primary cancer samples with adjacent normal breast tissues, 1,280 of the 1,844 detected proteins from the cell-free compartments were differentially expressed. Normal breast tissues were, in comparison to the PDSs, enriched for proteins involved in oxidation-reducing processes, secretion, regulation of exocytosis, and ECM organization (Supplementary Figure S2).</p><p>Next, we used k-means clustering to identify potential subgroups of patients based on the protein composition of the cell-free PDSs. PDS Clusters 1-3 were recognized, distinguished by the expression of proteins in Clusters A-C. Interestingly, the PDS clusters were significantly associated with cancer subtypes (Figure 1B and Supplementary Table S2). Cluster 1 was mainly derived from lobular cancers (63%) and low-grade cancers, showing high levels of 458 proteins involved in ECM organization, biological adhesion, and leukocyte-mediated immunity forming protein Cluster A. Cluster 2 was primarily derived from ductal cancers (77%) and showed pronounced expression of protein Cluster B, comprising of 396 proteins related to exocytosis, secretion and neutrophil degranulation. Cluster 3 included a mixture of ductal and lobular cancers with the highest levels of proteins from Cluster C, containing 990 proteins mainly involved in metabolic processes and establishment of cellular localization. When identifying proteins separating the two cancer types independently of the defined clusters (Figure 1C and Supplementary Table S3), ductal cancers were enriched for proteins classified as modifying enzymes, metabolite interconversion enzymes, RNA metabolism proteins and translational proteins. In contrast, lobular cancers showed high protein contents of ECM and defense/immunity proteins (Figure 1D), supporting earlier findings that subsets of lobular cancers might be more responsive to immune-targeting cancer therapies [<span>1</span>].</p><p>Next, we identified PDS-associated proteins that significantly differed between patients with or without recurrent disease (Figure 1E). The 52 proteins associated with progressive disease and recurrences were mainly classified as transporter and metabolite interconversion enzymes, while the 31 proteins linked to non-recurrent cancer primarily were cytoskeletal and scaffold/adaptor proteins. Interestingly, members of the keratin protein and solute carrier (SLC) families were prominent among the proteins associated with aggressive disease, and 8 out of 14 identified keratins were more abundant in PDSs from patients later having disease recurrences (Figure 1F). Higher levels of KRT78 in PDSs were significantly associated with poor disease-free survival in univariate (Figure 1G) as well as multivariable analyses (hazard ratio = 14.86, <i>P</i> = 0.01). In line with the presented data, keratins are abundantly expressed in subsets of epithelial cells and are linked to prognosis in many cancer types [<span>6</span>].</p><p>To further define the scaffold content in breast cancer, we clustered the PDSs based on a subset of 126 ECM-related proteins traditionally being representative of the TME (Figure 1H and Supplementary Table S4). Three new ECM-based PDS clusters were observed, only partly overlapping with the previous reported clusters (Supplementary Figure S3), and further significantly associated with cancer grade and age of the patients (Supplementary Tables S5-S6). Cluster ECM-1 showed a high proportion of low-grade cancers, mixed patient ages and was distinguished by high presence of collagens, microfibril-associated proteins (EMILIN1, MFAP2), fibrillins (FBN1, FBN2), latent transforming growth factor beta binding protein LTBP1, and peroxidin PRDX4, as well as low levels of integrin subunit ITGB2. Cluster ECM-2 was associated with high-grade cancer, older patient ages and was strongly associated with lower levels of ECM proteins, specifically collagens and laminin subunits, as well as of the structural protein tenascin XB (TNXB). In contrast, cluster ECM-3 mainly included low-grade cancers of all ages and was defined by higher ECM protein content. When detailing the collagen abundance in the PDSs in relation to patient age, there was a significant gradual decrease in 10 out of 21 detected collagens with increasing patient age (Figure 1I).</p><p>Proteins identified in the TME could be important when designing future in vitro three-dimensional (3D) growth models but could also be further evaluated as potential diagnostic biomarkers or even targets for cancer therapies. Importantly, the presented data demonstrate that ECM-related proteins were often more abundant in less malignant low-grade TME. This suggest that 3D growth models mimicking aggressive breast cancer cannot be recapitulated using only ECM proteins but should be complemented with other proteins present in the cancer niche. The age of the cancer patient was also associated with the ECM composition of the PDS, and younger patients exhibited higher level of ECM proteins, specifically collagens. The collagen turnover is a normal part of tissue homeostasis, and collagens commonly becomes more loose, disorganized, and fragmented in older tissues, including the skin [<span>7</span>]. Elderly patients also have different pharmacokinetic profiles compared to younger patients. Based on the obvious structural differences now also demonstrated in the TME, age-specific cancer drugs could be developed and tailored for managing varying malignant properties within the TME of younger or older cancer patients. Regarding the presence of intracellular proteins in the cell-free PDSs from breast cancer patients, other studies exploring ECM proteins in decellularized tissues [<span>8, 9</span>] also detected large amounts of intracellular proteins despite using harsh detergent treatments and enrichment processes. These results support that the multitude of proteins detected in this study indeed represents structurally incorporated and scaffold-associated proteins revealed by the PDS method. The results further suggest that different cell types within the TME are contributing to the imprinting of the scaffold structures, but future studies should detail the potential contribution from secreted and circulating factors.</p><p>In conclusion, the results suggest that breast cancers can be subclassified based on the levels of specific proteins in the cell-free PDS microenvironment. The PDS compositions were not only limited to ECM-associated proteins but also incorporated proteins linked to processes such as secretion, transport, localization, immune response, and metabolism. Importantly, properties of the PDSs were indeed linked to clinical characteristics of the cancer disease, suggesting that different qualities of the TME have the potential to add clinically relevant information for breast cancer.</p><p>A.S and G.L are shareholders and board members of iScaff Pharma AB. The approach using patient-derived scaffolds is patent pending (WO 2018/083231 A1). A.S is shareholder and board member of SiMSen Diagnostics and Tulebovaasta.</p><p>This work was supported by grants from The Swedish Research Council (2019-01273 and 2021-01008), Sweden's Innovation Agency (2017-03737), and Swedish Cancer Foundation (22-2214 and 22-2080), the Swedish state under the agreement between the Swedish government and county councils, the ALF-agreement (965065 and 965580) and BioCARE National Strategic Research Program at University of Gothenburg, Region Västra Götaland, The Sjöberg Foundation, Assar Gabrielssons Research Foundation, Stiftelsen Sigurd och Elsa Goljes Minne, and Kungliga och Hvitfeldtska Stiftelsen.</p><p>Patient consent to process patient material and data was waived for usage of biobanked materials by the Regional Ethics (Region Väst etiknämnd) Committee in Gothenburg, Seweden, while written consent was obtained from all patients donating fresh tissues (DNR: 515-12 and T972-18). Biobank samples were collected from 1980 to 1999 in Sweden, and patients were monitored until November 15, 2012. The study was performed in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines.</p>\",\"PeriodicalId\":9495,\"journal\":{\"name\":\"Cancer Communications\",\"volume\":\"44 6\",\"pages\":\"695-699\"},\"PeriodicalIF\":20.1000,\"publicationDate\":\"2024-04-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12542\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Communications\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12542\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Communications","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12542","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
Proteomics of cell-free breast cancer scaffolds identify clinically relevant imprinted proteins and cancer-progressing properties
The composition of the extracellular tumor microenvironment (TME) has not been fully delineated, limiting the understanding of general cancer-progressing properties within the cancer niche. The interplay and dynamics between cancer cells and the surrounding structures and cells clearly differ between various subtypes of cancer, adding to the complexity of precision medicine [1].
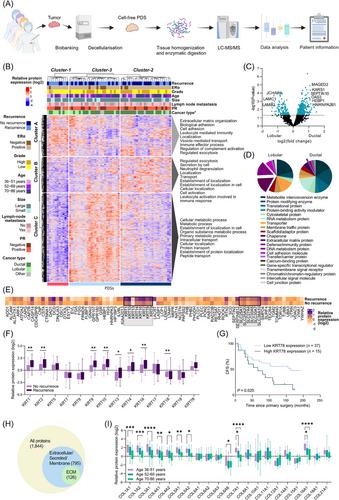
To better understand the composition and to define the imprinted proteins of the TME in breast cancer and its potential associations with clinical properties of the disease, we performed global proteomic analysis on a cohort of 63 decellularized patient-derived scaffolds (PDSs). PDSs represents the cell-free TME and were prepared using primary lesions from breast cancer patients with available clinicopathological data (Figure 1A, Supplementary file of methods). The PDS method has earlier been shown to maintain tumor tissue heterogeniety in vitro, producing quantitative assessments of the activity of the TME when studying cancer cell lines adapted to various PDS-based cell cultures [2]. Specific gene changes in the cancer population induced by the heterogenous PDS culture conditions have also been linked to clinical observations, validating the selected strategy for this study [2-5].
The analysis of the cell-free PDSs identified 1,844 unique proteins (Supplementary Table S1), showing enrichment for proteins related to metabolism, translation, transport, immunity, and extracellular matrix (ECM). Surprisingly, most proteins were annotated as cytoplasmic, suggesting that intracellular proteins were also associated with the PDSs, as further deliberated below (Supplementary Figure S1). When comparing the protein contents from primary cancer samples with adjacent normal breast tissues, 1,280 of the 1,844 detected proteins from the cell-free compartments were differentially expressed. Normal breast tissues were, in comparison to the PDSs, enriched for proteins involved in oxidation-reducing processes, secretion, regulation of exocytosis, and ECM organization (Supplementary Figure S2).
Next, we used k-means clustering to identify potential subgroups of patients based on the protein composition of the cell-free PDSs. PDS Clusters 1-3 were recognized, distinguished by the expression of proteins in Clusters A-C. Interestingly, the PDS clusters were significantly associated with cancer subtypes (Figure 1B and Supplementary Table S2). Cluster 1 was mainly derived from lobular cancers (63%) and low-grade cancers, showing high levels of 458 proteins involved in ECM organization, biological adhesion, and leukocyte-mediated immunity forming protein Cluster A. Cluster 2 was primarily derived from ductal cancers (77%) and showed pronounced expression of protein Cluster B, comprising of 396 proteins related to exocytosis, secretion and neutrophil degranulation. Cluster 3 included a mixture of ductal and lobular cancers with the highest levels of proteins from Cluster C, containing 990 proteins mainly involved in metabolic processes and establishment of cellular localization. When identifying proteins separating the two cancer types independently of the defined clusters (Figure 1C and Supplementary Table S3), ductal cancers were enriched for proteins classified as modifying enzymes, metabolite interconversion enzymes, RNA metabolism proteins and translational proteins. In contrast, lobular cancers showed high protein contents of ECM and defense/immunity proteins (Figure 1D), supporting earlier findings that subsets of lobular cancers might be more responsive to immune-targeting cancer therapies [1].
Next, we identified PDS-associated proteins that significantly differed between patients with or without recurrent disease (Figure 1E). The 52 proteins associated with progressive disease and recurrences were mainly classified as transporter and metabolite interconversion enzymes, while the 31 proteins linked to non-recurrent cancer primarily were cytoskeletal and scaffold/adaptor proteins. Interestingly, members of the keratin protein and solute carrier (SLC) families were prominent among the proteins associated with aggressive disease, and 8 out of 14 identified keratins were more abundant in PDSs from patients later having disease recurrences (Figure 1F). Higher levels of KRT78 in PDSs were significantly associated with poor disease-free survival in univariate (Figure 1G) as well as multivariable analyses (hazard ratio = 14.86, P = 0.01). In line with the presented data, keratins are abundantly expressed in subsets of epithelial cells and are linked to prognosis in many cancer types [6].
To further define the scaffold content in breast cancer, we clustered the PDSs based on a subset of 126 ECM-related proteins traditionally being representative of the TME (Figure 1H and Supplementary Table S4). Three new ECM-based PDS clusters were observed, only partly overlapping with the previous reported clusters (Supplementary Figure S3), and further significantly associated with cancer grade and age of the patients (Supplementary Tables S5-S6). Cluster ECM-1 showed a high proportion of low-grade cancers, mixed patient ages and was distinguished by high presence of collagens, microfibril-associated proteins (EMILIN1, MFAP2), fibrillins (FBN1, FBN2), latent transforming growth factor beta binding protein LTBP1, and peroxidin PRDX4, as well as low levels of integrin subunit ITGB2. Cluster ECM-2 was associated with high-grade cancer, older patient ages and was strongly associated with lower levels of ECM proteins, specifically collagens and laminin subunits, as well as of the structural protein tenascin XB (TNXB). In contrast, cluster ECM-3 mainly included low-grade cancers of all ages and was defined by higher ECM protein content. When detailing the collagen abundance in the PDSs in relation to patient age, there was a significant gradual decrease in 10 out of 21 detected collagens with increasing patient age (Figure 1I).
Proteins identified in the TME could be important when designing future in vitro three-dimensional (3D) growth models but could also be further evaluated as potential diagnostic biomarkers or even targets for cancer therapies. Importantly, the presented data demonstrate that ECM-related proteins were often more abundant in less malignant low-grade TME. This suggest that 3D growth models mimicking aggressive breast cancer cannot be recapitulated using only ECM proteins but should be complemented with other proteins present in the cancer niche. The age of the cancer patient was also associated with the ECM composition of the PDS, and younger patients exhibited higher level of ECM proteins, specifically collagens. The collagen turnover is a normal part of tissue homeostasis, and collagens commonly becomes more loose, disorganized, and fragmented in older tissues, including the skin [7]. Elderly patients also have different pharmacokinetic profiles compared to younger patients. Based on the obvious structural differences now also demonstrated in the TME, age-specific cancer drugs could be developed and tailored for managing varying malignant properties within the TME of younger or older cancer patients. Regarding the presence of intracellular proteins in the cell-free PDSs from breast cancer patients, other studies exploring ECM proteins in decellularized tissues [8, 9] also detected large amounts of intracellular proteins despite using harsh detergent treatments and enrichment processes. These results support that the multitude of proteins detected in this study indeed represents structurally incorporated and scaffold-associated proteins revealed by the PDS method. The results further suggest that different cell types within the TME are contributing to the imprinting of the scaffold structures, but future studies should detail the potential contribution from secreted and circulating factors.
In conclusion, the results suggest that breast cancers can be subclassified based on the levels of specific proteins in the cell-free PDS microenvironment. The PDS compositions were not only limited to ECM-associated proteins but also incorporated proteins linked to processes such as secretion, transport, localization, immune response, and metabolism. Importantly, properties of the PDSs were indeed linked to clinical characteristics of the cancer disease, suggesting that different qualities of the TME have the potential to add clinically relevant information for breast cancer.
A.S and G.L are shareholders and board members of iScaff Pharma AB. The approach using patient-derived scaffolds is patent pending (WO 2018/083231 A1). A.S is shareholder and board member of SiMSen Diagnostics and Tulebovaasta.
This work was supported by grants from The Swedish Research Council (2019-01273 and 2021-01008), Sweden's Innovation Agency (2017-03737), and Swedish Cancer Foundation (22-2214 and 22-2080), the Swedish state under the agreement between the Swedish government and county councils, the ALF-agreement (965065 and 965580) and BioCARE National Strategic Research Program at University of Gothenburg, Region Västra Götaland, The Sjöberg Foundation, Assar Gabrielssons Research Foundation, Stiftelsen Sigurd och Elsa Goljes Minne, and Kungliga och Hvitfeldtska Stiftelsen.
Patient consent to process patient material and data was waived for usage of biobanked materials by the Regional Ethics (Region Väst etiknämnd) Committee in Gothenburg, Seweden, while written consent was obtained from all patients donating fresh tissues (DNR: 515-12 and T972-18). Biobank samples were collected from 1980 to 1999 in Sweden, and patients were monitored until November 15, 2012. The study was performed in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines.
期刊介绍:
Cancer Communications is an open access, peer-reviewed online journal that encompasses basic, clinical, and translational cancer research. The journal welcomes submissions concerning clinical trials, epidemiology, molecular and cellular biology, and genetics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


