{"title":"日本患者左心室大小与心脏再同步化疗法结果的相互作用","authors":"Ryo Ito MD, PhD, Yusuke Kondo MD, PhD, FESC, Masahiro Nakano MD, PhD, Takatsugu Kajiyama MD, PhD, Miyo Nakano MD, PhD, Mari Kitagawa MD, PhD, Masafumi Sugawara MD, Toshinori Chiba MD, Yoshio Kobayashi MD, PhD","doi":"10.1002/clc.24267","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>We analyzed the influence of the QRS duration (QRSd) to LV end-diastolic volume (LVEDV) ratio on cardiac resynchronization therapy (CRT) outcomes in heart failure patients classified as III/IV per the New York Heart Association (NYHA) and with small body size.</p>\n </section>\n \n <section>\n \n <h3> Hypothesis</h3>\n \n <p>We proposed the hypothesis that the QRSd/LV size ratio is a better index of the CRT substrate.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We enrolled 114 patients with advanced heart failure (NYHA class III/IV, and LV ejection fraction >35%) who received a CRT device, including those with left bundle branch block (LBBB) and QRSd ≥120 milliseconds (<i>n</i> = 60), non-LBBB and QRSd ≥150 milliseconds (<i>n</i> = 30) and non-LBBB and QRSd of 120−149 milliseconds (<i>n</i> = 24).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Over a mean follow-up period of 65 ± 58 months, the incidence of the primary endpoint, a composite of all-cause death and hospitalization for heart failure, showed no significant intergroup difference (43.3% vs. 50.0% vs. 37.5%, respectively, <i>p</i> = .72). Similarly, among 104 patients with QRSd/LVEDV ≥ 0.67 (<i>n</i> = 54) and QRSd/LVEDV < 0.67 (<i>n</i> = 52), no significant differences were observed in the incidence of the primary endpoint (35.1% vs. 51.9%, <i>p</i> = .49). Nevertheless, patients with QRSd/LVEDV ≥ 0.67 showed better survival than those with QRSd/LVEDV < 0.67 (14.8% vs. 34.6%, <i>p</i> = .0024).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Advanced HF patients with a higher QRSd/LVEDV ratio showed better survival in this small-body–size population. Thus, the risk is concentrated among those with a larger QRSd, and patients with a relatively smaller left ventricular size appeared to benefit from CRT.</p>\n </section>\n </div>","PeriodicalId":2,"journal":{"name":"ACS Applied Bio Materials","volume":null,"pages":null},"PeriodicalIF":4.6000,"publicationDate":"2024-04-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24267","citationCount":"0","resultStr":"{\"title\":\"Interaction of left ventricular size with the outcome of cardiac resynchronization therapy in Japanese patients\",\"authors\":\"Ryo Ito MD, PhD, Yusuke Kondo MD, PhD, FESC, Masahiro Nakano MD, PhD, Takatsugu Kajiyama MD, PhD, Miyo Nakano MD, PhD, Mari Kitagawa MD, PhD, Masafumi Sugawara MD, Toshinori Chiba MD, Yoshio Kobayashi MD, PhD\",\"doi\":\"10.1002/clc.24267\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>We analyzed the influence of the QRS duration (QRSd) to LV end-diastolic volume (LVEDV) ratio on cardiac resynchronization therapy (CRT) outcomes in heart failure patients classified as III/IV per the New York Heart Association (NYHA) and with small body size.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Hypothesis</h3>\\n \\n <p>We proposed the hypothesis that the QRSd/LV size ratio is a better index of the CRT substrate.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We enrolled 114 patients with advanced heart failure (NYHA class III/IV, and LV ejection fraction >35%) who received a CRT device, including those with left bundle branch block (LBBB) and QRSd ≥120 milliseconds (<i>n</i> = 60), non-LBBB and QRSd ≥150 milliseconds (<i>n</i> = 30) and non-LBBB and QRSd of 120−149 milliseconds (<i>n</i> = 24).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Over a mean follow-up period of 65 ± 58 months, the incidence of the primary endpoint, a composite of all-cause death and hospitalization for heart failure, showed no significant intergroup difference (43.3% vs. 50.0% vs. 37.5%, respectively, <i>p</i> = .72). Similarly, among 104 patients with QRSd/LVEDV ≥ 0.67 (<i>n</i> = 54) and QRSd/LVEDV < 0.67 (<i>n</i> = 52), no significant differences were observed in the incidence of the primary endpoint (35.1% vs. 51.9%, <i>p</i> = .49). Nevertheless, patients with QRSd/LVEDV ≥ 0.67 showed better survival than those with QRSd/LVEDV < 0.67 (14.8% vs. 34.6%, <i>p</i> = .0024).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Advanced HF patients with a higher QRSd/LVEDV ratio showed better survival in this small-body–size population. Thus, the risk is concentrated among those with a larger QRSd, and patients with a relatively smaller left ventricular size appeared to benefit from CRT.</p>\\n </section>\\n </div>\",\"PeriodicalId\":2,\"journal\":{\"name\":\"ACS Applied Bio Materials\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2024-04-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24267\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACS Applied Bio Materials\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clc.24267\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MATERIALS SCIENCE, BIOMATERIALS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Bio Materials","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.24267","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MATERIALS SCIENCE, BIOMATERIALS","Score":null,"Total":0}
Interaction of left ventricular size with the outcome of cardiac resynchronization therapy in Japanese patients
Background
We analyzed the influence of the QRS duration (QRSd) to LV end-diastolic volume (LVEDV) ratio on cardiac resynchronization therapy (CRT) outcomes in heart failure patients classified as III/IV per the New York Heart Association (NYHA) and with small body size.
Hypothesis
We proposed the hypothesis that the QRSd/LV size ratio is a better index of the CRT substrate.
Methods
We enrolled 114 patients with advanced heart failure (NYHA class III/IV, and LV ejection fraction >35%) who received a CRT device, including those with left bundle branch block (LBBB) and QRSd ≥120 milliseconds (n = 60), non-LBBB and QRSd ≥150 milliseconds (n = 30) and non-LBBB and QRSd of 120−149 milliseconds (n = 24).
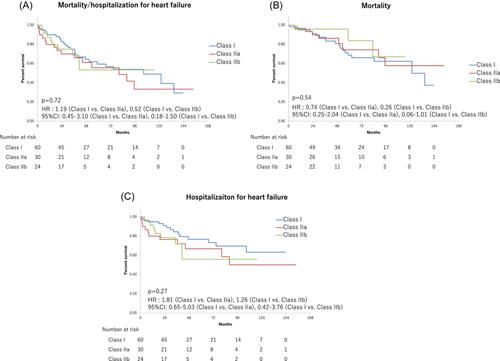
Results
Over a mean follow-up period of 65 ± 58 months, the incidence of the primary endpoint, a composite of all-cause death and hospitalization for heart failure, showed no significant intergroup difference (43.3% vs. 50.0% vs. 37.5%, respectively, p = .72). Similarly, among 104 patients with QRSd/LVEDV ≥ 0.67 (n = 54) and QRSd/LVEDV < 0.67 (n = 52), no significant differences were observed in the incidence of the primary endpoint (35.1% vs. 51.9%, p = .49). Nevertheless, patients with QRSd/LVEDV ≥ 0.67 showed better survival than those with QRSd/LVEDV < 0.67 (14.8% vs. 34.6%, p = .0024).
Conclusion
Advanced HF patients with a higher QRSd/LVEDV ratio showed better survival in this small-body–size population. Thus, the risk is concentrated among those with a larger QRSd, and patients with a relatively smaller left ventricular size appeared to benefit from CRT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


