Xiao-Bin Zheng MM, Hai-Yan Wu MM, Ming Zhang MM, Bing-Qi Yao MM
{"title":"下壁心肌梗死患者 V1 导联 R 波振幅和基底下心肌梗死的临床意义。","authors":"Xiao-Bin Zheng MM, Hai-Yan Wu MM, Ming Zhang MM, Bing-Qi Yao MM","doi":"10.1111/anec.13114","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>To assess electrocardiogram (ECG) for risk stratification in inferior ST-elevation myocardial infarction (STEMI) patients within 24 h.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Three hundred thirty-four patients were divided into four ECG-based groups: Group A: R V<sub>1</sub> <0.3 mV with ST-segment elevation (ST↑) V<sub>7</sub>–V<sub>9</sub>, Group B: R V<sub>1</sub> <0.3 mV without ST↑ V<sub>7</sub>–V<sub>9</sub>, Group C: R V<sub>1</sub> ≥0.3 mV with ST↑ V<sub>7</sub>–V<sub>9</sub>, and Group D: R V<sub>1</sub> ≥0.3 mV without ST↑ V<sub>7</sub>–V<sub>9</sub>.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Group A demonstrated the longest QRS duration, followed by Groups B, C, and D. ECG signs for right ventricle (RV) infarction were more common in Groups A and B (<i>p</i> < .01). ST elevation in V<sub>6</sub>, indicative of left ventricle (LV) lateral injury, was more higher in Group C than in Group A, while the ∑ST↑ V<sub>3</sub>R + V<sub>4</sub>R + V<sub>5</sub>R, representing RV infarction, showed the opposite trend (<i>p</i> < .05). The estimated LV infarct size from ECG was similar between Groups A and C, yet Group A had higher creatine kinase MB isoform (CK-MB; <i>p</i> < .05). Cardiac troponin I (cTNI) was higher in Groups A and C than in B and D (<i>p</i> < .05 and <i>p</i> = .16, respectively). NT-proBNP decreased across groups (<i>p</i> = .20), with the highest left ventricular ejection fraction (LVEF) observed in Group D (<i>p</i> < .05). Group A notably demonstrated more cardiac dysfunction within 4 h post-onset.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>For inferior STEMI patients, concurrent R V<sub>1</sub> <0.3 mV with ST↑ V<sub>7</sub>–V<sub>9</sub> suggests prolonged ventricular activation and notable myocardial damage. RV infarction's dominance over LV lateral injury might explain these observations.</p>\n </section>\n </div>","PeriodicalId":8074,"journal":{"name":"Annals of Noninvasive Electrocardiology","volume":"29 3","pages":""},"PeriodicalIF":1.1000,"publicationDate":"2024-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anec.13114","citationCount":"0","resultStr":"{\"title\":\"Clinical significance of R-wave amplitude in lead V1 and inferobasal myocardial infarction in patients with inferior wall myocardial infarction\",\"authors\":\"Xiao-Bin Zheng MM, Hai-Yan Wu MM, Ming Zhang MM, Bing-Qi Yao MM\",\"doi\":\"10.1111/anec.13114\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>To assess electrocardiogram (ECG) for risk stratification in inferior ST-elevation myocardial infarction (STEMI) patients within 24 h.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Three hundred thirty-four patients were divided into four ECG-based groups: Group A: R V<sub>1</sub> <0.3 mV with ST-segment elevation (ST↑) V<sub>7</sub>–V<sub>9</sub>, Group B: R V<sub>1</sub> <0.3 mV without ST↑ V<sub>7</sub>–V<sub>9</sub>, Group C: R V<sub>1</sub> ≥0.3 mV with ST↑ V<sub>7</sub>–V<sub>9</sub>, and Group D: R V<sub>1</sub> ≥0.3 mV without ST↑ V<sub>7</sub>–V<sub>9</sub>.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Group A demonstrated the longest QRS duration, followed by Groups B, C, and D. ECG signs for right ventricle (RV) infarction were more common in Groups A and B (<i>p</i> < .01). ST elevation in V<sub>6</sub>, indicative of left ventricle (LV) lateral injury, was more higher in Group C than in Group A, while the ∑ST↑ V<sub>3</sub>R + V<sub>4</sub>R + V<sub>5</sub>R, representing RV infarction, showed the opposite trend (<i>p</i> < .05). The estimated LV infarct size from ECG was similar between Groups A and C, yet Group A had higher creatine kinase MB isoform (CK-MB; <i>p</i> < .05). Cardiac troponin I (cTNI) was higher in Groups A and C than in B and D (<i>p</i> < .05 and <i>p</i> = .16, respectively). NT-proBNP decreased across groups (<i>p</i> = .20), with the highest left ventricular ejection fraction (LVEF) observed in Group D (<i>p</i> < .05). Group A notably demonstrated more cardiac dysfunction within 4 h post-onset.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>For inferior STEMI patients, concurrent R V<sub>1</sub> <0.3 mV with ST↑ V<sub>7</sub>–V<sub>9</sub> suggests prolonged ventricular activation and notable myocardial damage. RV infarction's dominance over LV lateral injury might explain these observations.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8074,\"journal\":{\"name\":\"Annals of Noninvasive Electrocardiology\",\"volume\":\"29 3\",\"pages\":\"\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2024-04-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anec.13114\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Noninvasive Electrocardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/anec.13114\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Noninvasive Electrocardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/anec.13114","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Clinical significance of R-wave amplitude in lead V1 and inferobasal myocardial infarction in patients with inferior wall myocardial infarction
Objective
To assess electrocardiogram (ECG) for risk stratification in inferior ST-elevation myocardial infarction (STEMI) patients within 24 h.
Methods
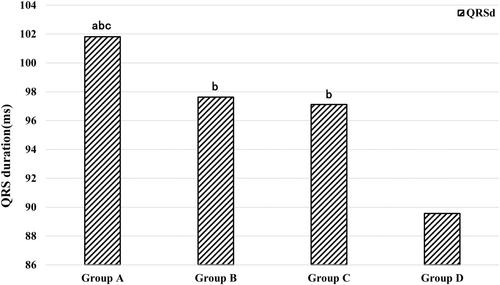
Three hundred thirty-four patients were divided into four ECG-based groups: Group A: R V1 <0.3 mV with ST-segment elevation (ST↑) V7–V9, Group B: R V1 <0.3 mV without ST↑ V7–V9, Group C: R V1 ≥0.3 mV with ST↑ V7–V9, and Group D: R V1 ≥0.3 mV without ST↑ V7–V9.
Results
Group A demonstrated the longest QRS duration, followed by Groups B, C, and D. ECG signs for right ventricle (RV) infarction were more common in Groups A and B (p < .01). ST elevation in V6, indicative of left ventricle (LV) lateral injury, was more higher in Group C than in Group A, while the ∑ST↑ V3R + V4R + V5R, representing RV infarction, showed the opposite trend (p < .05). The estimated LV infarct size from ECG was similar between Groups A and C, yet Group A had higher creatine kinase MB isoform (CK-MB; p < .05). Cardiac troponin I (cTNI) was higher in Groups A and C than in B and D (p < .05 and p = .16, respectively). NT-proBNP decreased across groups (p = .20), with the highest left ventricular ejection fraction (LVEF) observed in Group D (p < .05). Group A notably demonstrated more cardiac dysfunction within 4 h post-onset.
Conclusions
For inferior STEMI patients, concurrent R V1 <0.3 mV with ST↑ V7–V9 suggests prolonged ventricular activation and notable myocardial damage. RV infarction's dominance over LV lateral injury might explain these observations.
期刊介绍:
The ANNALS OF NONINVASIVE ELECTROCARDIOLOGY (A.N.E) is an online only journal that incorporates ongoing advances in the clinical application and technology of traditional and new ECG-based techniques in the diagnosis and treatment of cardiac patients.
ANE is the first journal in an evolving subspecialty that incorporates ongoing advances in the clinical application and technology of traditional and new ECG-based techniques in the diagnosis and treatment of cardiac patients. The publication includes topics related to 12-lead, exercise and high-resolution electrocardiography, arrhythmias, ischemia, repolarization phenomena, heart rate variability, circadian rhythms, bioengineering technology, signal-averaged ECGs, T-wave alternans and automatic external defibrillation.
ANE publishes peer-reviewed articles of interest to clinicians and researchers in the field of noninvasive electrocardiology. Original research, clinical studies, state-of-the-art reviews, case reports, technical notes, and letters to the editors will be published to meet future demands in this field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


