Cecilia Rorsman, Maiwand Farouq, Sofia Marinko, Pyotr G Platonov, Rasmus Borgquist
{"title":"接受起搏器、再同步化治疗或除颤器植入的已知心衰患者的年龄分层临床结果。","authors":"Cecilia Rorsman, Maiwand Farouq, Sofia Marinko, Pyotr G Platonov, Rasmus Borgquist","doi":"10.1159/000538529","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Patients with heart failure (HF) and bradycardia may be eligible for different types of cardiac implantable electronic devices (CIED), depending on the presence of atrioventricular conduction disease, age, and comorbidities. We aimed to assess the prognosis for these patients, after CIED implantation, stratified for the type of CIED device.</p><p><strong>Methods: </strong>All patients with preexisting HF diagnosis who received a CIED with a right ventricular lead during the period 2005-2018 in Sweden were identified via the pacemaker registry. Data were crossmatched with the population registry and national disease registries. The outcome was 5-year risk of HF hospitalization and mortality.</p><p><strong>Results: </strong>A total of 37,745 patients were included in the study. Comparing demographics for implantable cardioverter defibrillator versus pacemaker implants, median age was 66 years versus 83 years, 20% versus 41% were female, 64% versus 50% had ischemic heart disease, and 35% versus 67% had atrial fibrillation (all p < 0.001). Five-year mortality was highest in single-chamber pacemaker recipients (61% compared to average 40%, p < 0.001), but the proportion of cardiovascular mortality was highest for cardiac resynchronization therapy (CRT) recipients (68% vs. 63% p < 0.001). Adjusted mortality was higher for pacemaker patients in all age decile groups (ranging from <60 to >90 years old, all p < 0.001), HF hospitalization occurred in 28% (dual-chamber pacemaker) to 39% (CRT-P) of patients, and cause of death was HF in 15% (dual-chamber pacemaker) to 25% (CRT-D), all p < 0.001.</p><p><strong>Conclusion: </strong>In this large real-world cohort of CIED-treated patients with prior HF, demography and mortality data indicate that clinicians chose devices according to the overall status of the patient. HF-related events occurred in all groups but were more common in CRT-treated patients.</p>","PeriodicalId":9391,"journal":{"name":"Cardiology","volume":" ","pages":"474-483"},"PeriodicalIF":1.7000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11449187/pdf/","citationCount":"0","resultStr":"{\"title\":\"Age-Stratified Clinical Outcome in Patients with Known Heart Failure Who Receive Pacemaker, Resynchronization Therapy, or Defibrillator Implants.\",\"authors\":\"Cecilia Rorsman, Maiwand Farouq, Sofia Marinko, Pyotr G Platonov, Rasmus Borgquist\",\"doi\":\"10.1159/000538529\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Patients with heart failure (HF) and bradycardia may be eligible for different types of cardiac implantable electronic devices (CIED), depending on the presence of atrioventricular conduction disease, age, and comorbidities. We aimed to assess the prognosis for these patients, after CIED implantation, stratified for the type of CIED device.</p><p><strong>Methods: </strong>All patients with preexisting HF diagnosis who received a CIED with a right ventricular lead during the period 2005-2018 in Sweden were identified via the pacemaker registry. Data were crossmatched with the population registry and national disease registries. The outcome was 5-year risk of HF hospitalization and mortality.</p><p><strong>Results: </strong>A total of 37,745 patients were included in the study. Comparing demographics for implantable cardioverter defibrillator versus pacemaker implants, median age was 66 years versus 83 years, 20% versus 41% were female, 64% versus 50% had ischemic heart disease, and 35% versus 67% had atrial fibrillation (all p < 0.001). Five-year mortality was highest in single-chamber pacemaker recipients (61% compared to average 40%, p < 0.001), but the proportion of cardiovascular mortality was highest for cardiac resynchronization therapy (CRT) recipients (68% vs. 63% p < 0.001). Adjusted mortality was higher for pacemaker patients in all age decile groups (ranging from <60 to >90 years old, all p < 0.001), HF hospitalization occurred in 28% (dual-chamber pacemaker) to 39% (CRT-P) of patients, and cause of death was HF in 15% (dual-chamber pacemaker) to 25% (CRT-D), all p < 0.001.</p><p><strong>Conclusion: </strong>In this large real-world cohort of CIED-treated patients with prior HF, demography and mortality data indicate that clinicians chose devices according to the overall status of the patient. HF-related events occurred in all groups but were more common in CRT-treated patients.</p>\",\"PeriodicalId\":9391,\"journal\":{\"name\":\"Cardiology\",\"volume\":\" \",\"pages\":\"474-483\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11449187/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000538529\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000538529","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Age-Stratified Clinical Outcome in Patients with Known Heart Failure Who Receive Pacemaker, Resynchronization Therapy, or Defibrillator Implants.
Introduction: Patients with heart failure (HF) and bradycardia may be eligible for different types of cardiac implantable electronic devices (CIED), depending on the presence of atrioventricular conduction disease, age, and comorbidities. We aimed to assess the prognosis for these patients, after CIED implantation, stratified for the type of CIED device.
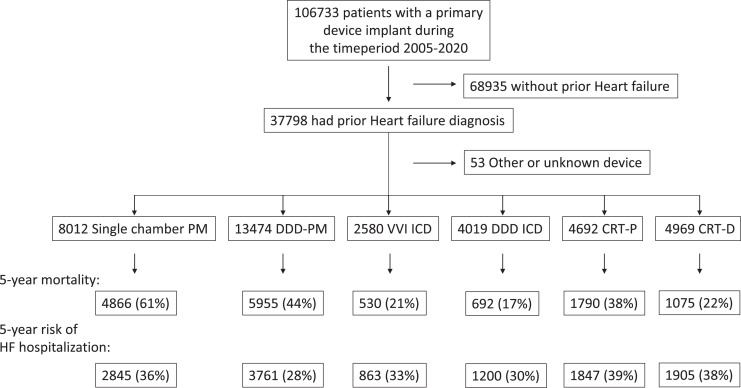
Methods: All patients with preexisting HF diagnosis who received a CIED with a right ventricular lead during the period 2005-2018 in Sweden were identified via the pacemaker registry. Data were crossmatched with the population registry and national disease registries. The outcome was 5-year risk of HF hospitalization and mortality.
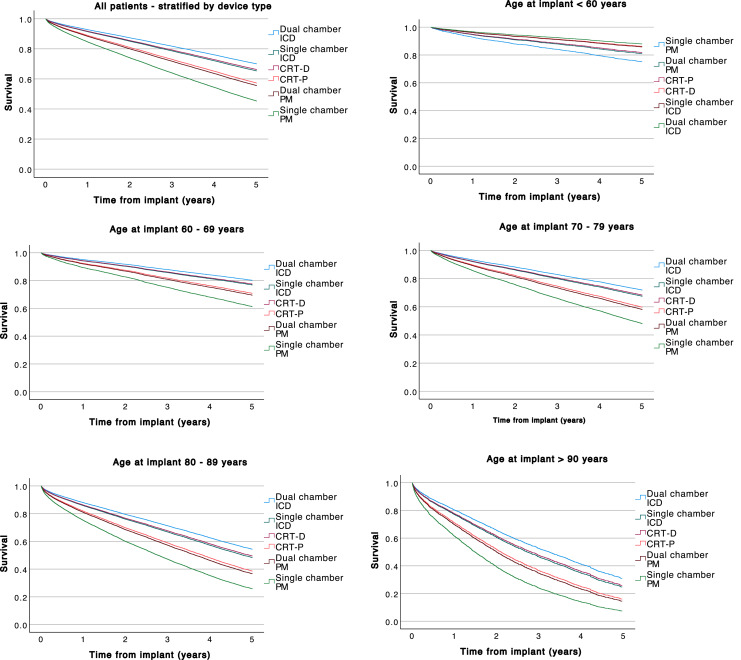
Results: A total of 37,745 patients were included in the study. Comparing demographics for implantable cardioverter defibrillator versus pacemaker implants, median age was 66 years versus 83 years, 20% versus 41% were female, 64% versus 50% had ischemic heart disease, and 35% versus 67% had atrial fibrillation (all p < 0.001). Five-year mortality was highest in single-chamber pacemaker recipients (61% compared to average 40%, p < 0.001), but the proportion of cardiovascular mortality was highest for cardiac resynchronization therapy (CRT) recipients (68% vs. 63% p < 0.001). Adjusted mortality was higher for pacemaker patients in all age decile groups (ranging from <60 to >90 years old, all p < 0.001), HF hospitalization occurred in 28% (dual-chamber pacemaker) to 39% (CRT-P) of patients, and cause of death was HF in 15% (dual-chamber pacemaker) to 25% (CRT-D), all p < 0.001.
Conclusion: In this large real-world cohort of CIED-treated patients with prior HF, demography and mortality data indicate that clinicians chose devices according to the overall status of the patient. HF-related events occurred in all groups but were more common in CRT-treated patients.
期刊介绍:
''Cardiology'' features first reports on original clinical, preclinical and fundamental research as well as ''Novel Insights from Clinical Experience'' and topical comprehensive reviews in selected areas of cardiovascular disease. ''Editorial Comments'' provide a critical but positive evaluation of a recent article. Papers not only describe but offer critical appraisals of new developments in non-invasive and invasive diagnostic methods and in pharmacologic, nutritional and mechanical/surgical therapies. Readers are thus kept informed of current strategies in the prevention, recognition and treatment of heart disease. Special sections in a variety of subspecialty areas reinforce the journal''s value as a complete record of recent progress for all cardiologists, internists, cardiac surgeons, clinical physiologists, pharmacologists and professionals in other areas of medicine interested in current activity in cardiovascular diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


