Haiyang Zhou, Jiahui Yin, Anqi Wang, Xiaomao Yin, Taojun Jin, Kai Xu, Lin Zhu, Jiexuan Wang, Wenqiang Wang, Wei Zhang, Xinxiang Li, Zhiqian Hu, Xinxing Li
{"title":"转移性结直肠癌患者恶性腹水的单细胞图谱。","authors":"Haiyang Zhou, Jiahui Yin, Anqi Wang, Xiaomao Yin, Taojun Jin, Kai Xu, Lin Zhu, Jiexuan Wang, Wenqiang Wang, Wei Zhang, Xinxiang Li, Zhiqian Hu, Xinxing Li","doi":"10.1002/cac2.12541","DOIUrl":null,"url":null,"abstract":"<p>The presence of malignant ascites in colorectal cancer (CRC) patients is associated with a poor prognosis, a high risk of recurrence, and resistance to chemotherapy and immune therapy [<span>1-3</span>]. Understanding the complex interactions among different kinds of cells and the ecosystem of peritoneal metastasized colorectal cancer (pmCRC) ascites may provide insights into effective treatment strategies.</p><p>We profiled the single-cell transcriptomes of 96,065 cells from ascites samples of 12 treatment-naïve patients with pmCRC using the 10× single-cell RNA-sequencing (scRNA-seq) (Supplementary Figure S1A, Supplementary Table S1). Eleven major cell types were identified by characteristic canonical cell markers, including epithelial cells, endothelial cells, fibroblasts, T cells, B cells, monocytes, macrophages, plasma cells, natural killer (NK) cells, dendritic cells (DCs), and mast cells (Figure 1A-B). The main cellular components of pmCRC ascites are T cells (40,095; 41.7%), macrophages (28,487; 29.7%), and fibroblasts (5,932; 6.2%). Compared with primary CRC, which showed 14.8% epithelial cells [<span>4</span>], only 0.3% (291) epithelial cells were found in the ascites. The low percentage of epithelial cells in pmCRC ascites was consistent with the scRNA-seq studies of another tumor ascites [<span>5-7</span>].</p><p>We classified the 12 patients into 2 groups according to their treatment response as follows: 8 patients (P02, P03, P04, P07, P08, P09, P11, and P12) had stable disease (SD), while 4 (P01, P05, P06, and P10) had progressive disease (PD). Single-cell transcriptomic analyses have revealed high heterogeneity of cell composition in 12 patients. The SD group exhibited a higher proportion of fibroblasts and epithelial cells (Figure 1B). Remarkably, fibroblasts had significantly different expression characteristics between the 2 groups (Figure 1C), and the top five upregulated/downregulated genes were visualized in 11 cell types (Figure 1D). We also found a significant increase in the frequency of macrophages in pmCRC ascites compared with the primary tumors [<span>4</span>] (Figure 1E). It hinted that significant inter-patient variability in the composition and functional programs of pmCRC ascites cells under different disease states.</p><p>To comprehensively study the cellular interactions within the pmCRC ascites ecosystem, we predicted cell-cell communication networks using CellChat. Overall, we identified 44 significant ligand-receptor pair interactions. Although T cells were the most abundant cell population (41.7%) in pmCRC ascites, fibroblasts and macrophages were the core of the cellular interaction network (Figure 1F), suggesting their important roles in recruiting and cross-talking with diverse cells in the pmCRC ascites ecosystem.</p><p>The result of cellular communications suggested that there was a complex interplay between various signaling molecule. Macrophage migration inhibitory factor (MIF), annexin, complement, and C-C chemokine ligand (CCL) were the most active outgoing/incoming signaling molecules in CRC ascites (Supplementary Figure S1B). Fibroblasts directly contacted with different types of cells via ligand-receptor interactions of the MIF-(CD74 + C-X-C chemokine receptor type 4 [CXCR4]) and MIF-(CD74 + CD44) axes and C3-(integrin alpha X [ITGAX] + integrin subunit beta 2 [ITGB2]) (Figure 1G). Notably, macrophage populations were more likely to interact with other cells through the adhesive ligand-receptor pairs galectin-9 (LGALS9)-CD44 and LGALS9-CD45, which were not observed in other cell populations (Figure 1G). CD74, LGALS9 were significantly associated with metastasis in The Cancer Genome Atlas (TCGA) CRC cohorts. We also found CD44 and ITGAX were survival (Figure 1H; CD44 and ITGAX showed no significant differential expression between metastatic and non-metastatic patients, so data are not shown). These results indicated that the entire cellular interaction network of pmCRC ascites contributed to establishing an immunosuppressive and metastatic microenvironment.</p><p>We observed that the abundance of fibroblasts in pmCRC ascites samples was significantly greater in SD patients than in PD patients (Figure 1B). The fibroblasts were partitioned into 7 distinct clusters (C0-C6) based on unsupervised clustering (Figure 1I). All sub-clusters of cancer-associated fibroblasts (CAfs) showed a high expression of extracellular matrix cancer-associated fibroblasts (eCAFs) signature (Figure 1J), while inflammatory CAF (iCAF), myofibroblast CAF (myCAF), matrix CAF (mCAF), and vascular CAF (vCAF) only presented in a small fraction of fibroblasts (Supplementary Figure S1C), supporting the role of eCAFs in enhancing the metastatic potential of pmCRC. A higher abundance of antigen-presenting cancer-associated fibroblasts (apCAFs) was observed in the PD cohort (<i>n</i> = 310) than in the SD cohort (<i>n</i> = 93) (Wilcoxon test, <i>P</i> = 0.049). These results indicated that the CAFs in pmCRC ascites have bidirectional associations with immune regulation function, serving as a favorable candidate for CRC treatment. Differentially expressed genes and gene ontology (GO) analyses showed that the “cell-cell adhesion”, “inflammatory response”, and “cytokine production” were differentially enriched between primary tumors and ascites (Supplementary Figure S1D), which implied that the liquid state of ascites changed the functions of the fibroblast populations.</p><p>Macrophages were significantly enriched in pmCRC ascites and categorized into 8 sub-clusters (C0-C7) (Figure 1K). Using the previously defined “M1” and “M2” signatures, C2 showed an “M1-like” pattern, and C5 showed “M2-like” patterns. We also identified a small sub-cluster of C5 co-expressed both “M1” and “M2” gene signatures (Figure 1L), which have been reported in previous studies on solid tumors [<span>8</span>]. We next examined the expression of a series of the previously reported immunosuppressive genes (leukocyte-associated immunoglobulin-like receptor 1 [LAIR1], hepatitis A virus cellular receptor 2 [HAVCR2; also known as T cell immunoglobulin and mucin domain-containing protein 3], LGALS9, and V-set immunoregulatory receptor [VSIR]) in macrophage sub-clusters. Because the expression pattern of the “M2” marker gene CD163 perfectly coincided with that of LAIR1 in all sub-clusters (Figure 1M), we postulated that the immunosuppressive function of tumor-associated macrophages (TAMs) might be exerted via LAIR1. Two other immunosuppressive genes, T cell immune receptor with Ig and ITIM domains (TIGIT) and programmed cell death 1 (PDCD1), were also identified highly expressed in C5. C4 highly expressed the key immunosuppressive phenotypic marker triggering receptor expressed on myeloid cells 2 (TREM2) (Figure 1N). In summary, the majority of macrophages in pmCRC ascites exhibited high immunosuppressive features.</p><p>We identified 11 sub-clusters of T cells according to the expression of their respective markers, including CD4<sup>+</sup> T cells (C1, C4, C5, and C6) and CD8<sup>+</sup> T cells (C0, C2, C3, C7, C8, C9, and C10) (Figure 1O). Most CD8<sup>+</sup> effector memory cells re-expressing CD45RA T (Temra/Teff) cells (C8) were from patient 5 (P05), and CD8<sup>+</sup> effector memory T (Tem) cells (C7) were mostly from patient 8 (P08); the remaining 10 patients exhibited high heterogeneity in 11 T-cell sub-clusters (Supplementary Figure S1E-F). Importantly, CD8<sup>+</sup> tissue-resident memory (Trm) cells (C7), which were reported to be associated with forming a tertiary lymphoid structure (TLS) [<span>9</span>], were less abundant in SD patients (P03, P08, P09, P11, and P12). We also observed that all sub-clusters expressed ferritin light chain (FTL) (Supplementary Figure S1G), which was reported to regulate chemoresistance and metastasis in CRC [<span>10</span>]. We calculated the cytotoxicity, proliferation, and exhaustion signatures for all CD8<sup>+</sup> T-cell sub-clusters (Figure 1P). Only one sub-cluster of CD8<sup>+</sup> T cells was not show exhaustion signature (C10). Clusters 9 and 10 exhibited slightly higher proliferation, which could recruit cytotoxic T cells. The abundance of C9 and C10 was low, suggesting that T cells may play a minor role in the immune microenvironment of ascites and may work synergistically with other cell populations. Moreover, we predicted immunomodulatory drugs targeting macrophages, where gene sets were extracted from the macrophages of the pmCRC ascites data (Figure 1Q).</p><p>In conclusion, we found that T cells, fibroblasts, and macrophages exhibited immunosuppressive features in pmCRC ascites (Figure 1R). The cellular landscape of pmCRC ascites has the significant indication of patients’ immune status, providing insights for prognosis and therapy selection.</p><p>Haiyang Zhou made contributions to the conceptualization, funding acquisition, investigation, resource acquisition, and writing original draft.</p><p>Jiahui Yin made contributions to the data curation, formal analysis, and software analysis.</p><p>Anqi Wang made contributions to the formal analysis, investigation, and resource acquisition.</p><p>Xiaomao Yin made contributions to the formal analysis.</p><p>Taojun Jin made contributions to the formal analysis and visualization.</p><p>Kai Xu made contributions to the resource acquisition and supervision.</p><p>Lin Zhu made contributions to the investigation and resource acquisition.</p><p>Jiexuan Wang made contributions to the investigation and resources acquisition.</p><p>Wenqiang Wang made contributions to the resource acquisition.</p><p>Wei Zhang made contributions to the resource acquisition.</p><p>Xinxiang Li made contributions to the conceptualization, visualization, and writing—review & editing.</p><p>Zhiqian Hu made contributions to the funding acquisition, visualization, and writing—review & editing.</p><p>Xinxing Li made contributions to the investigation, resource acquisition, visualization, writing—original draft, and writing—review & editing.</p><p>All authors read and approved the final manuscript.</p><p>The authors declare that they have no competing interests.</p><p>The authors gratefully acknowledge the financial support from the National Key R&D Program of China (No. 2019YFA0110601), National Natural Science Foundation of China (No. 81571827), Natural Science Foundation Project of Shanghai Science and Technology Commission (SKW2030), Excellent Discipline Reserve Talent Plan of Tongji Hospital Affiliated to Tongji University (HBRC2014), Clinical research Project of Tongji Hospital Affiliated to Tongji University (ITJ-ZD-2104), Key talent introduction project of Tongji Hospital Affiliated to Tongji University (RCQD2102), Talent project of Tongji Hospital Affiliated to Tongji University (GJPY2111), and Shanghai Tongji Hospital special disease database construction project (TJ-DB-2105).</p><p>All the investigation protocols were approved by the Institutional Ethics Committees of Shanghai Changzheng Hospital and Shanghai Tongji Hospital (SBKT-2022-155). All subjects provided informed consent to participate in the study and approved the use of their biological samples for analysis. All experiments were performed following institutional guidelines, in compliance with relevant laws. Data sharing mechanisms will ensure that the rights and privacy of individuals participating in research will be guaranteed.</p>","PeriodicalId":9495,"journal":{"name":"Cancer Communications","volume":"44 7","pages":"713-717"},"PeriodicalIF":20.1000,"publicationDate":"2024-03-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11260760/pdf/","citationCount":"0","resultStr":"{\"title\":\"Single-cell landscape of malignant ascites from patients with metastatic colorectal cancer\",\"authors\":\"Haiyang Zhou, Jiahui Yin, Anqi Wang, Xiaomao Yin, Taojun Jin, Kai Xu, Lin Zhu, Jiexuan Wang, Wenqiang Wang, Wei Zhang, Xinxiang Li, Zhiqian Hu, Xinxing Li\",\"doi\":\"10.1002/cac2.12541\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The presence of malignant ascites in colorectal cancer (CRC) patients is associated with a poor prognosis, a high risk of recurrence, and resistance to chemotherapy and immune therapy [<span>1-3</span>]. Understanding the complex interactions among different kinds of cells and the ecosystem of peritoneal metastasized colorectal cancer (pmCRC) ascites may provide insights into effective treatment strategies.</p><p>We profiled the single-cell transcriptomes of 96,065 cells from ascites samples of 12 treatment-naïve patients with pmCRC using the 10× single-cell RNA-sequencing (scRNA-seq) (Supplementary Figure S1A, Supplementary Table S1). Eleven major cell types were identified by characteristic canonical cell markers, including epithelial cells, endothelial cells, fibroblasts, T cells, B cells, monocytes, macrophages, plasma cells, natural killer (NK) cells, dendritic cells (DCs), and mast cells (Figure 1A-B). The main cellular components of pmCRC ascites are T cells (40,095; 41.7%), macrophages (28,487; 29.7%), and fibroblasts (5,932; 6.2%). Compared with primary CRC, which showed 14.8% epithelial cells [<span>4</span>], only 0.3% (291) epithelial cells were found in the ascites. The low percentage of epithelial cells in pmCRC ascites was consistent with the scRNA-seq studies of another tumor ascites [<span>5-7</span>].</p><p>We classified the 12 patients into 2 groups according to their treatment response as follows: 8 patients (P02, P03, P04, P07, P08, P09, P11, and P12) had stable disease (SD), while 4 (P01, P05, P06, and P10) had progressive disease (PD). Single-cell transcriptomic analyses have revealed high heterogeneity of cell composition in 12 patients. The SD group exhibited a higher proportion of fibroblasts and epithelial cells (Figure 1B). Remarkably, fibroblasts had significantly different expression characteristics between the 2 groups (Figure 1C), and the top five upregulated/downregulated genes were visualized in 11 cell types (Figure 1D). We also found a significant increase in the frequency of macrophages in pmCRC ascites compared with the primary tumors [<span>4</span>] (Figure 1E). It hinted that significant inter-patient variability in the composition and functional programs of pmCRC ascites cells under different disease states.</p><p>To comprehensively study the cellular interactions within the pmCRC ascites ecosystem, we predicted cell-cell communication networks using CellChat. Overall, we identified 44 significant ligand-receptor pair interactions. Although T cells were the most abundant cell population (41.7%) in pmCRC ascites, fibroblasts and macrophages were the core of the cellular interaction network (Figure 1F), suggesting their important roles in recruiting and cross-talking with diverse cells in the pmCRC ascites ecosystem.</p><p>The result of cellular communications suggested that there was a complex interplay between various signaling molecule. Macrophage migration inhibitory factor (MIF), annexin, complement, and C-C chemokine ligand (CCL) were the most active outgoing/incoming signaling molecules in CRC ascites (Supplementary Figure S1B). Fibroblasts directly contacted with different types of cells via ligand-receptor interactions of the MIF-(CD74 + C-X-C chemokine receptor type 4 [CXCR4]) and MIF-(CD74 + CD44) axes and C3-(integrin alpha X [ITGAX] + integrin subunit beta 2 [ITGB2]) (Figure 1G). Notably, macrophage populations were more likely to interact with other cells through the adhesive ligand-receptor pairs galectin-9 (LGALS9)-CD44 and LGALS9-CD45, which were not observed in other cell populations (Figure 1G). CD74, LGALS9 were significantly associated with metastasis in The Cancer Genome Atlas (TCGA) CRC cohorts. We also found CD44 and ITGAX were survival (Figure 1H; CD44 and ITGAX showed no significant differential expression between metastatic and non-metastatic patients, so data are not shown). These results indicated that the entire cellular interaction network of pmCRC ascites contributed to establishing an immunosuppressive and metastatic microenvironment.</p><p>We observed that the abundance of fibroblasts in pmCRC ascites samples was significantly greater in SD patients than in PD patients (Figure 1B). The fibroblasts were partitioned into 7 distinct clusters (C0-C6) based on unsupervised clustering (Figure 1I). All sub-clusters of cancer-associated fibroblasts (CAfs) showed a high expression of extracellular matrix cancer-associated fibroblasts (eCAFs) signature (Figure 1J), while inflammatory CAF (iCAF), myofibroblast CAF (myCAF), matrix CAF (mCAF), and vascular CAF (vCAF) only presented in a small fraction of fibroblasts (Supplementary Figure S1C), supporting the role of eCAFs in enhancing the metastatic potential of pmCRC. A higher abundance of antigen-presenting cancer-associated fibroblasts (apCAFs) was observed in the PD cohort (<i>n</i> = 310) than in the SD cohort (<i>n</i> = 93) (Wilcoxon test, <i>P</i> = 0.049). These results indicated that the CAFs in pmCRC ascites have bidirectional associations with immune regulation function, serving as a favorable candidate for CRC treatment. Differentially expressed genes and gene ontology (GO) analyses showed that the “cell-cell adhesion”, “inflammatory response”, and “cytokine production” were differentially enriched between primary tumors and ascites (Supplementary Figure S1D), which implied that the liquid state of ascites changed the functions of the fibroblast populations.</p><p>Macrophages were significantly enriched in pmCRC ascites and categorized into 8 sub-clusters (C0-C7) (Figure 1K). Using the previously defined “M1” and “M2” signatures, C2 showed an “M1-like” pattern, and C5 showed “M2-like” patterns. We also identified a small sub-cluster of C5 co-expressed both “M1” and “M2” gene signatures (Figure 1L), which have been reported in previous studies on solid tumors [<span>8</span>]. We next examined the expression of a series of the previously reported immunosuppressive genes (leukocyte-associated immunoglobulin-like receptor 1 [LAIR1], hepatitis A virus cellular receptor 2 [HAVCR2; also known as T cell immunoglobulin and mucin domain-containing protein 3], LGALS9, and V-set immunoregulatory receptor [VSIR]) in macrophage sub-clusters. Because the expression pattern of the “M2” marker gene CD163 perfectly coincided with that of LAIR1 in all sub-clusters (Figure 1M), we postulated that the immunosuppressive function of tumor-associated macrophages (TAMs) might be exerted via LAIR1. Two other immunosuppressive genes, T cell immune receptor with Ig and ITIM domains (TIGIT) and programmed cell death 1 (PDCD1), were also identified highly expressed in C5. C4 highly expressed the key immunosuppressive phenotypic marker triggering receptor expressed on myeloid cells 2 (TREM2) (Figure 1N). In summary, the majority of macrophages in pmCRC ascites exhibited high immunosuppressive features.</p><p>We identified 11 sub-clusters of T cells according to the expression of their respective markers, including CD4<sup>+</sup> T cells (C1, C4, C5, and C6) and CD8<sup>+</sup> T cells (C0, C2, C3, C7, C8, C9, and C10) (Figure 1O). Most CD8<sup>+</sup> effector memory cells re-expressing CD45RA T (Temra/Teff) cells (C8) were from patient 5 (P05), and CD8<sup>+</sup> effector memory T (Tem) cells (C7) were mostly from patient 8 (P08); the remaining 10 patients exhibited high heterogeneity in 11 T-cell sub-clusters (Supplementary Figure S1E-F). Importantly, CD8<sup>+</sup> tissue-resident memory (Trm) cells (C7), which were reported to be associated with forming a tertiary lymphoid structure (TLS) [<span>9</span>], were less abundant in SD patients (P03, P08, P09, P11, and P12). We also observed that all sub-clusters expressed ferritin light chain (FTL) (Supplementary Figure S1G), which was reported to regulate chemoresistance and metastasis in CRC [<span>10</span>]. We calculated the cytotoxicity, proliferation, and exhaustion signatures for all CD8<sup>+</sup> T-cell sub-clusters (Figure 1P). Only one sub-cluster of CD8<sup>+</sup> T cells was not show exhaustion signature (C10). Clusters 9 and 10 exhibited slightly higher proliferation, which could recruit cytotoxic T cells. The abundance of C9 and C10 was low, suggesting that T cells may play a minor role in the immune microenvironment of ascites and may work synergistically with other cell populations. Moreover, we predicted immunomodulatory drugs targeting macrophages, where gene sets were extracted from the macrophages of the pmCRC ascites data (Figure 1Q).</p><p>In conclusion, we found that T cells, fibroblasts, and macrophages exhibited immunosuppressive features in pmCRC ascites (Figure 1R). The cellular landscape of pmCRC ascites has the significant indication of patients’ immune status, providing insights for prognosis and therapy selection.</p><p>Haiyang Zhou made contributions to the conceptualization, funding acquisition, investigation, resource acquisition, and writing original draft.</p><p>Jiahui Yin made contributions to the data curation, formal analysis, and software analysis.</p><p>Anqi Wang made contributions to the formal analysis, investigation, and resource acquisition.</p><p>Xiaomao Yin made contributions to the formal analysis.</p><p>Taojun Jin made contributions to the formal analysis and visualization.</p><p>Kai Xu made contributions to the resource acquisition and supervision.</p><p>Lin Zhu made contributions to the investigation and resource acquisition.</p><p>Jiexuan Wang made contributions to the investigation and resources acquisition.</p><p>Wenqiang Wang made contributions to the resource acquisition.</p><p>Wei Zhang made contributions to the resource acquisition.</p><p>Xinxiang Li made contributions to the conceptualization, visualization, and writing—review & editing.</p><p>Zhiqian Hu made contributions to the funding acquisition, visualization, and writing—review & editing.</p><p>Xinxing Li made contributions to the investigation, resource acquisition, visualization, writing—original draft, and writing—review & editing.</p><p>All authors read and approved the final manuscript.</p><p>The authors declare that they have no competing interests.</p><p>The authors gratefully acknowledge the financial support from the National Key R&D Program of China (No. 2019YFA0110601), National Natural Science Foundation of China (No. 81571827), Natural Science Foundation Project of Shanghai Science and Technology Commission (SKW2030), Excellent Discipline Reserve Talent Plan of Tongji Hospital Affiliated to Tongji University (HBRC2014), Clinical research Project of Tongji Hospital Affiliated to Tongji University (ITJ-ZD-2104), Key talent introduction project of Tongji Hospital Affiliated to Tongji University (RCQD2102), Talent project of Tongji Hospital Affiliated to Tongji University (GJPY2111), and Shanghai Tongji Hospital special disease database construction project (TJ-DB-2105).</p><p>All the investigation protocols were approved by the Institutional Ethics Committees of Shanghai Changzheng Hospital and Shanghai Tongji Hospital (SBKT-2022-155). All subjects provided informed consent to participate in the study and approved the use of their biological samples for analysis. All experiments were performed following institutional guidelines, in compliance with relevant laws. Data sharing mechanisms will ensure that the rights and privacy of individuals participating in research will be guaranteed.</p>\",\"PeriodicalId\":9495,\"journal\":{\"name\":\"Cancer Communications\",\"volume\":\"44 7\",\"pages\":\"713-717\"},\"PeriodicalIF\":20.1000,\"publicationDate\":\"2024-03-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11260760/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Communications\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12541\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Communications","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12541","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
Single-cell landscape of malignant ascites from patients with metastatic colorectal cancer
The presence of malignant ascites in colorectal cancer (CRC) patients is associated with a poor prognosis, a high risk of recurrence, and resistance to chemotherapy and immune therapy [1-3]. Understanding the complex interactions among different kinds of cells and the ecosystem of peritoneal metastasized colorectal cancer (pmCRC) ascites may provide insights into effective treatment strategies.
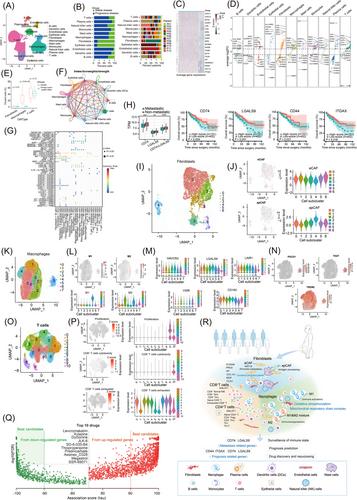
We profiled the single-cell transcriptomes of 96,065 cells from ascites samples of 12 treatment-naïve patients with pmCRC using the 10× single-cell RNA-sequencing (scRNA-seq) (Supplementary Figure S1A, Supplementary Table S1). Eleven major cell types were identified by characteristic canonical cell markers, including epithelial cells, endothelial cells, fibroblasts, T cells, B cells, monocytes, macrophages, plasma cells, natural killer (NK) cells, dendritic cells (DCs), and mast cells (Figure 1A-B). The main cellular components of pmCRC ascites are T cells (40,095; 41.7%), macrophages (28,487; 29.7%), and fibroblasts (5,932; 6.2%). Compared with primary CRC, which showed 14.8% epithelial cells [4], only 0.3% (291) epithelial cells were found in the ascites. The low percentage of epithelial cells in pmCRC ascites was consistent with the scRNA-seq studies of another tumor ascites [5-7].
We classified the 12 patients into 2 groups according to their treatment response as follows: 8 patients (P02, P03, P04, P07, P08, P09, P11, and P12) had stable disease (SD), while 4 (P01, P05, P06, and P10) had progressive disease (PD). Single-cell transcriptomic analyses have revealed high heterogeneity of cell composition in 12 patients. The SD group exhibited a higher proportion of fibroblasts and epithelial cells (Figure 1B). Remarkably, fibroblasts had significantly different expression characteristics between the 2 groups (Figure 1C), and the top five upregulated/downregulated genes were visualized in 11 cell types (Figure 1D). We also found a significant increase in the frequency of macrophages in pmCRC ascites compared with the primary tumors [4] (Figure 1E). It hinted that significant inter-patient variability in the composition and functional programs of pmCRC ascites cells under different disease states.
To comprehensively study the cellular interactions within the pmCRC ascites ecosystem, we predicted cell-cell communication networks using CellChat. Overall, we identified 44 significant ligand-receptor pair interactions. Although T cells were the most abundant cell population (41.7%) in pmCRC ascites, fibroblasts and macrophages were the core of the cellular interaction network (Figure 1F), suggesting their important roles in recruiting and cross-talking with diverse cells in the pmCRC ascites ecosystem.
The result of cellular communications suggested that there was a complex interplay between various signaling molecule. Macrophage migration inhibitory factor (MIF), annexin, complement, and C-C chemokine ligand (CCL) were the most active outgoing/incoming signaling molecules in CRC ascites (Supplementary Figure S1B). Fibroblasts directly contacted with different types of cells via ligand-receptor interactions of the MIF-(CD74 + C-X-C chemokine receptor type 4 [CXCR4]) and MIF-(CD74 + CD44) axes and C3-(integrin alpha X [ITGAX] + integrin subunit beta 2 [ITGB2]) (Figure 1G). Notably, macrophage populations were more likely to interact with other cells through the adhesive ligand-receptor pairs galectin-9 (LGALS9)-CD44 and LGALS9-CD45, which were not observed in other cell populations (Figure 1G). CD74, LGALS9 were significantly associated with metastasis in The Cancer Genome Atlas (TCGA) CRC cohorts. We also found CD44 and ITGAX were survival (Figure 1H; CD44 and ITGAX showed no significant differential expression between metastatic and non-metastatic patients, so data are not shown). These results indicated that the entire cellular interaction network of pmCRC ascites contributed to establishing an immunosuppressive and metastatic microenvironment.
We observed that the abundance of fibroblasts in pmCRC ascites samples was significantly greater in SD patients than in PD patients (Figure 1B). The fibroblasts were partitioned into 7 distinct clusters (C0-C6) based on unsupervised clustering (Figure 1I). All sub-clusters of cancer-associated fibroblasts (CAfs) showed a high expression of extracellular matrix cancer-associated fibroblasts (eCAFs) signature (Figure 1J), while inflammatory CAF (iCAF), myofibroblast CAF (myCAF), matrix CAF (mCAF), and vascular CAF (vCAF) only presented in a small fraction of fibroblasts (Supplementary Figure S1C), supporting the role of eCAFs in enhancing the metastatic potential of pmCRC. A higher abundance of antigen-presenting cancer-associated fibroblasts (apCAFs) was observed in the PD cohort (n = 310) than in the SD cohort (n = 93) (Wilcoxon test, P = 0.049). These results indicated that the CAFs in pmCRC ascites have bidirectional associations with immune regulation function, serving as a favorable candidate for CRC treatment. Differentially expressed genes and gene ontology (GO) analyses showed that the “cell-cell adhesion”, “inflammatory response”, and “cytokine production” were differentially enriched between primary tumors and ascites (Supplementary Figure S1D), which implied that the liquid state of ascites changed the functions of the fibroblast populations.
Macrophages were significantly enriched in pmCRC ascites and categorized into 8 sub-clusters (C0-C7) (Figure 1K). Using the previously defined “M1” and “M2” signatures, C2 showed an “M1-like” pattern, and C5 showed “M2-like” patterns. We also identified a small sub-cluster of C5 co-expressed both “M1” and “M2” gene signatures (Figure 1L), which have been reported in previous studies on solid tumors [8]. We next examined the expression of a series of the previously reported immunosuppressive genes (leukocyte-associated immunoglobulin-like receptor 1 [LAIR1], hepatitis A virus cellular receptor 2 [HAVCR2; also known as T cell immunoglobulin and mucin domain-containing protein 3], LGALS9, and V-set immunoregulatory receptor [VSIR]) in macrophage sub-clusters. Because the expression pattern of the “M2” marker gene CD163 perfectly coincided with that of LAIR1 in all sub-clusters (Figure 1M), we postulated that the immunosuppressive function of tumor-associated macrophages (TAMs) might be exerted via LAIR1. Two other immunosuppressive genes, T cell immune receptor with Ig and ITIM domains (TIGIT) and programmed cell death 1 (PDCD1), were also identified highly expressed in C5. C4 highly expressed the key immunosuppressive phenotypic marker triggering receptor expressed on myeloid cells 2 (TREM2) (Figure 1N). In summary, the majority of macrophages in pmCRC ascites exhibited high immunosuppressive features.
We identified 11 sub-clusters of T cells according to the expression of their respective markers, including CD4+ T cells (C1, C4, C5, and C6) and CD8+ T cells (C0, C2, C3, C7, C8, C9, and C10) (Figure 1O). Most CD8+ effector memory cells re-expressing CD45RA T (Temra/Teff) cells (C8) were from patient 5 (P05), and CD8+ effector memory T (Tem) cells (C7) were mostly from patient 8 (P08); the remaining 10 patients exhibited high heterogeneity in 11 T-cell sub-clusters (Supplementary Figure S1E-F). Importantly, CD8+ tissue-resident memory (Trm) cells (C7), which were reported to be associated with forming a tertiary lymphoid structure (TLS) [9], were less abundant in SD patients (P03, P08, P09, P11, and P12). We also observed that all sub-clusters expressed ferritin light chain (FTL) (Supplementary Figure S1G), which was reported to regulate chemoresistance and metastasis in CRC [10]. We calculated the cytotoxicity, proliferation, and exhaustion signatures for all CD8+ T-cell sub-clusters (Figure 1P). Only one sub-cluster of CD8+ T cells was not show exhaustion signature (C10). Clusters 9 and 10 exhibited slightly higher proliferation, which could recruit cytotoxic T cells. The abundance of C9 and C10 was low, suggesting that T cells may play a minor role in the immune microenvironment of ascites and may work synergistically with other cell populations. Moreover, we predicted immunomodulatory drugs targeting macrophages, where gene sets were extracted from the macrophages of the pmCRC ascites data (Figure 1Q).
In conclusion, we found that T cells, fibroblasts, and macrophages exhibited immunosuppressive features in pmCRC ascites (Figure 1R). The cellular landscape of pmCRC ascites has the significant indication of patients’ immune status, providing insights for prognosis and therapy selection.
Haiyang Zhou made contributions to the conceptualization, funding acquisition, investigation, resource acquisition, and writing original draft.
Jiahui Yin made contributions to the data curation, formal analysis, and software analysis.
Anqi Wang made contributions to the formal analysis, investigation, and resource acquisition.
Xiaomao Yin made contributions to the formal analysis.
Taojun Jin made contributions to the formal analysis and visualization.
Kai Xu made contributions to the resource acquisition and supervision.
Lin Zhu made contributions to the investigation and resource acquisition.
Jiexuan Wang made contributions to the investigation and resources acquisition.
Wenqiang Wang made contributions to the resource acquisition.
Wei Zhang made contributions to the resource acquisition.
Xinxiang Li made contributions to the conceptualization, visualization, and writing—review & editing.
Zhiqian Hu made contributions to the funding acquisition, visualization, and writing—review & editing.
Xinxing Li made contributions to the investigation, resource acquisition, visualization, writing—original draft, and writing—review & editing.
All authors read and approved the final manuscript.
The authors declare that they have no competing interests.
The authors gratefully acknowledge the financial support from the National Key R&D Program of China (No. 2019YFA0110601), National Natural Science Foundation of China (No. 81571827), Natural Science Foundation Project of Shanghai Science and Technology Commission (SKW2030), Excellent Discipline Reserve Talent Plan of Tongji Hospital Affiliated to Tongji University (HBRC2014), Clinical research Project of Tongji Hospital Affiliated to Tongji University (ITJ-ZD-2104), Key talent introduction project of Tongji Hospital Affiliated to Tongji University (RCQD2102), Talent project of Tongji Hospital Affiliated to Tongji University (GJPY2111), and Shanghai Tongji Hospital special disease database construction project (TJ-DB-2105).
All the investigation protocols were approved by the Institutional Ethics Committees of Shanghai Changzheng Hospital and Shanghai Tongji Hospital (SBKT-2022-155). All subjects provided informed consent to participate in the study and approved the use of their biological samples for analysis. All experiments were performed following institutional guidelines, in compliance with relevant laws. Data sharing mechanisms will ensure that the rights and privacy of individuals participating in research will be guaranteed.
期刊介绍:
Cancer Communications is an open access, peer-reviewed online journal that encompasses basic, clinical, and translational cancer research. The journal welcomes submissions concerning clinical trials, epidemiology, molecular and cellular biology, and genetics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


