Timothy J W Dawes, Valentine Woodham, Emma Sharkey, Angus McEwan, Graham Derrick, Vivek Muthurangu, Shahin Moledina, Lucy Hepburn
{"title":"利用超声心动图预测接受心导管检查的特发性肺动脉高压患儿术前心肺不良事件:一项队列研究。","authors":"Timothy J W Dawes, Valentine Woodham, Emma Sharkey, Angus McEwan, Graham Derrick, Vivek Muthurangu, Shahin Moledina, Lucy Hepburn","doi":"10.1007/s00246-024-03447-3","DOIUrl":null,"url":null,"abstract":"<p><p>General anesthesia in children with idiopathic pulmonary arterial hypertension (PAH) carries an increased risk of peri-operative cardiorespiratory complications though risk stratifying individual children pre-operatively remains difficult. We report the incidence and echocardiographic risk factors for adverse events in children with PAH undergoing general anesthesia for cardiac catheterization. Echocardiographic, hemodynamic, and adverse event data from consecutive PAH patients are reported. A multivariable predictive model was developed from echocardiographic variables identified by Bayesian univariable logistic regression. Model performance was reported by area under the curve for receiver operating characteristics (AUC<sub>roc</sub>) and precision/recall (AUC<sub>pr</sub>) and a pre-operative scoring system derived (0-100). Ninety-three children underwent 158 cardiac catheterizations with mean age 8.8 ± 4.6 years. Adverse events (n = 42) occurred in 15 patients (16%) during 16 catheterizations (10%) including cardiopulmonary resuscitation (n = 5, 3%), electrocardiographic changes (n = 3, 2%), significant hypotension (n = 2, 1%), stridor (n = 1, 1%), and death (n = 2, 1%). A multivariable model (age, right ventricular dysfunction, and dilatation, pulmonary and tricuspid regurgitation severity, and maximal velocity) was highly predictive of adverse events (AUC<sub>roc</sub> 0.86, 95% CI 0.75 to 1.00; AUC<sub>pr</sub> 0.68, 95% CI 0.50 to 0.91; baseline AUC<sub>pr</sub> 0.10). Pre-operative risk scores were higher in those who had a subsequent adverse event (median 47, IQR 43 to 53) than in those who did not (median 23, IQR 15 to 33). Pre-operative echocardiography informs the risk of peri-operative adverse events and may therefore be useful both for consent and multi-disciplinary care planning.</p>","PeriodicalId":19814,"journal":{"name":"Pediatric Cardiology","volume":" ","pages":"475-484"},"PeriodicalIF":1.5000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11787273/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predicting Peri-Operative Cardiorespiratory Adverse Events in Children with Idiopathic Pulmonary Arterial Hypertension Undergoing Cardiac Catheterization Using Echocardiography: A Cohort Study.\",\"authors\":\"Timothy J W Dawes, Valentine Woodham, Emma Sharkey, Angus McEwan, Graham Derrick, Vivek Muthurangu, Shahin Moledina, Lucy Hepburn\",\"doi\":\"10.1007/s00246-024-03447-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>General anesthesia in children with idiopathic pulmonary arterial hypertension (PAH) carries an increased risk of peri-operative cardiorespiratory complications though risk stratifying individual children pre-operatively remains difficult. We report the incidence and echocardiographic risk factors for adverse events in children with PAH undergoing general anesthesia for cardiac catheterization. Echocardiographic, hemodynamic, and adverse event data from consecutive PAH patients are reported. A multivariable predictive model was developed from echocardiographic variables identified by Bayesian univariable logistic regression. Model performance was reported by area under the curve for receiver operating characteristics (AUC<sub>roc</sub>) and precision/recall (AUC<sub>pr</sub>) and a pre-operative scoring system derived (0-100). Ninety-three children underwent 158 cardiac catheterizations with mean age 8.8 ± 4.6 years. Adverse events (n = 42) occurred in 15 patients (16%) during 16 catheterizations (10%) including cardiopulmonary resuscitation (n = 5, 3%), electrocardiographic changes (n = 3, 2%), significant hypotension (n = 2, 1%), stridor (n = 1, 1%), and death (n = 2, 1%). A multivariable model (age, right ventricular dysfunction, and dilatation, pulmonary and tricuspid regurgitation severity, and maximal velocity) was highly predictive of adverse events (AUC<sub>roc</sub> 0.86, 95% CI 0.75 to 1.00; AUC<sub>pr</sub> 0.68, 95% CI 0.50 to 0.91; baseline AUC<sub>pr</sub> 0.10). Pre-operative risk scores were higher in those who had a subsequent adverse event (median 47, IQR 43 to 53) than in those who did not (median 23, IQR 15 to 33). Pre-operative echocardiography informs the risk of peri-operative adverse events and may therefore be useful both for consent and multi-disciplinary care planning.</p>\",\"PeriodicalId\":19814,\"journal\":{\"name\":\"Pediatric Cardiology\",\"volume\":\" \",\"pages\":\"475-484\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11787273/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00246-024-03447-3\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00246-024-03447-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/21 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Predicting Peri-Operative Cardiorespiratory Adverse Events in Children with Idiopathic Pulmonary Arterial Hypertension Undergoing Cardiac Catheterization Using Echocardiography: A Cohort Study.
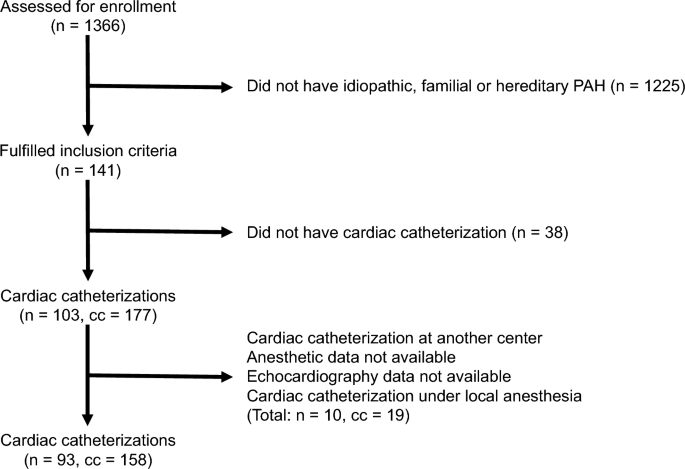
General anesthesia in children with idiopathic pulmonary arterial hypertension (PAH) carries an increased risk of peri-operative cardiorespiratory complications though risk stratifying individual children pre-operatively remains difficult. We report the incidence and echocardiographic risk factors for adverse events in children with PAH undergoing general anesthesia for cardiac catheterization. Echocardiographic, hemodynamic, and adverse event data from consecutive PAH patients are reported. A multivariable predictive model was developed from echocardiographic variables identified by Bayesian univariable logistic regression. Model performance was reported by area under the curve for receiver operating characteristics (AUCroc) and precision/recall (AUCpr) and a pre-operative scoring system derived (0-100). Ninety-three children underwent 158 cardiac catheterizations with mean age 8.8 ± 4.6 years. Adverse events (n = 42) occurred in 15 patients (16%) during 16 catheterizations (10%) including cardiopulmonary resuscitation (n = 5, 3%), electrocardiographic changes (n = 3, 2%), significant hypotension (n = 2, 1%), stridor (n = 1, 1%), and death (n = 2, 1%). A multivariable model (age, right ventricular dysfunction, and dilatation, pulmonary and tricuspid regurgitation severity, and maximal velocity) was highly predictive of adverse events (AUCroc 0.86, 95% CI 0.75 to 1.00; AUCpr 0.68, 95% CI 0.50 to 0.91; baseline AUCpr 0.10). Pre-operative risk scores were higher in those who had a subsequent adverse event (median 47, IQR 43 to 53) than in those who did not (median 23, IQR 15 to 33). Pre-operative echocardiography informs the risk of peri-operative adverse events and may therefore be useful both for consent and multi-disciplinary care planning.
期刊介绍:
The editor of Pediatric Cardiology welcomes original manuscripts concerning all aspects of heart disease in infants, children, and adolescents, including embryology and anatomy, physiology and pharmacology, biochemistry, pathology, genetics, radiology, clinical aspects, investigative cardiology, electrophysiology and echocardiography, and cardiac surgery. Articles which may include original articles, review articles, letters to the editor etc., must be written in English and must be submitted solely to Pediatric Cardiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


