{"title":"继发于 Blinatumomab 治疗的吉罗韦氏肺囊虫肺炎:病例报告。","authors":"Yue Yin, Kaini Shen, Hanyu Li, Lu Zhang","doi":"10.1159/000538256","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>With the increasing use of blinatumomab in relapsed or refractory B-cell precursor acute lymphoblastic leukemia (ALL), including minimal residual disease (MRD)-positive cases, awareness of its adverse effects has gradually improved. Pneumocystis jirovecii pneumonia (PCP) associated with blinatumomab therapy is rare.</p><p><strong>Case presentation: </strong>We present a case of PCP in a patient undergoing blinatumomab therapy. A 70-year-old female diagnosed with Philadelphia-like CRLF2 overexpression B-cell precursor ALL received blinatumomab as consolidation therapy after achieving complete remission with prior induction chemotherapy. On the second day of blinatumomab infusion, she developed intermittent low-grade fever, and chest computed tomography (CT) revealed subtle infiltrates and nodules. Despite empiric trimethoprim-sulfamethoxazole (TMP-SMX) prophylaxis, she progressed to significant shortness of breath and type I respiratory failure, with increased lactate dehydrogenase and β-D-glucan assays. Chest CT showed diffuse ground-glass opacities with scattered small nodules. The dry cough prompted next-generation sequencing of peripheral blood, which tested positive for pneumocystis jirovecii without evidence of other pathogens. Consequently, the patient was diagnosed with PCP. The first cycle of blinatumomab had to be discontinued, and therapeutic dosages of TMP-SMX and dexamethasone were administered, resulting in full recovery and stable condition during follow-ups.</p><p><strong>Conclusion: </strong>PCP is rare in B-cell precursor ALL patients receiving blinatumomab therapy but manifests with early onset and rapid disease progression. Despite prophylaxis, PCP infection cannot be ignored during blinatumomab therapy. Therefore, heightened attention is warranted when using blinatumomab therapy.</p>","PeriodicalId":10047,"journal":{"name":"Chemotherapy","volume":" ","pages":"104-107"},"PeriodicalIF":1.7000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11152014/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pneumocystis jirovecii Pneumonia Secondary to Blinatumomab Therapy: A Case Report.\",\"authors\":\"Yue Yin, Kaini Shen, Hanyu Li, Lu Zhang\",\"doi\":\"10.1159/000538256\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>With the increasing use of blinatumomab in relapsed or refractory B-cell precursor acute lymphoblastic leukemia (ALL), including minimal residual disease (MRD)-positive cases, awareness of its adverse effects has gradually improved. Pneumocystis jirovecii pneumonia (PCP) associated with blinatumomab therapy is rare.</p><p><strong>Case presentation: </strong>We present a case of PCP in a patient undergoing blinatumomab therapy. A 70-year-old female diagnosed with Philadelphia-like CRLF2 overexpression B-cell precursor ALL received blinatumomab as consolidation therapy after achieving complete remission with prior induction chemotherapy. On the second day of blinatumomab infusion, she developed intermittent low-grade fever, and chest computed tomography (CT) revealed subtle infiltrates and nodules. Despite empiric trimethoprim-sulfamethoxazole (TMP-SMX) prophylaxis, she progressed to significant shortness of breath and type I respiratory failure, with increased lactate dehydrogenase and β-D-glucan assays. Chest CT showed diffuse ground-glass opacities with scattered small nodules. The dry cough prompted next-generation sequencing of peripheral blood, which tested positive for pneumocystis jirovecii without evidence of other pathogens. Consequently, the patient was diagnosed with PCP. The first cycle of blinatumomab had to be discontinued, and therapeutic dosages of TMP-SMX and dexamethasone were administered, resulting in full recovery and stable condition during follow-ups.</p><p><strong>Conclusion: </strong>PCP is rare in B-cell precursor ALL patients receiving blinatumomab therapy but manifests with early onset and rapid disease progression. Despite prophylaxis, PCP infection cannot be ignored during blinatumomab therapy. Therefore, heightened attention is warranted when using blinatumomab therapy.</p>\",\"PeriodicalId\":10047,\"journal\":{\"name\":\"Chemotherapy\",\"volume\":\" \",\"pages\":\"104-107\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11152014/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Chemotherapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000538256\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chemotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000538256","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Pneumocystis jirovecii Pneumonia Secondary to Blinatumomab Therapy: A Case Report.
Introduction: With the increasing use of blinatumomab in relapsed or refractory B-cell precursor acute lymphoblastic leukemia (ALL), including minimal residual disease (MRD)-positive cases, awareness of its adverse effects has gradually improved. Pneumocystis jirovecii pneumonia (PCP) associated with blinatumomab therapy is rare.
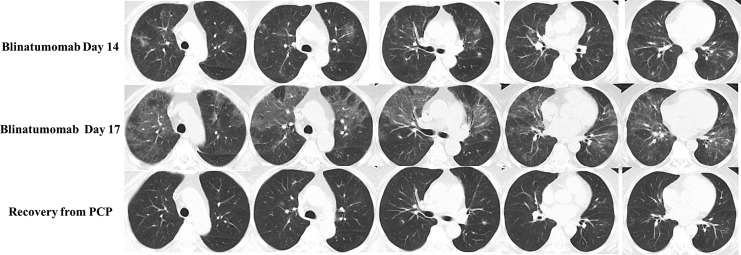
Case presentation: We present a case of PCP in a patient undergoing blinatumomab therapy. A 70-year-old female diagnosed with Philadelphia-like CRLF2 overexpression B-cell precursor ALL received blinatumomab as consolidation therapy after achieving complete remission with prior induction chemotherapy. On the second day of blinatumomab infusion, she developed intermittent low-grade fever, and chest computed tomography (CT) revealed subtle infiltrates and nodules. Despite empiric trimethoprim-sulfamethoxazole (TMP-SMX) prophylaxis, she progressed to significant shortness of breath and type I respiratory failure, with increased lactate dehydrogenase and β-D-glucan assays. Chest CT showed diffuse ground-glass opacities with scattered small nodules. The dry cough prompted next-generation sequencing of peripheral blood, which tested positive for pneumocystis jirovecii without evidence of other pathogens. Consequently, the patient was diagnosed with PCP. The first cycle of blinatumomab had to be discontinued, and therapeutic dosages of TMP-SMX and dexamethasone were administered, resulting in full recovery and stable condition during follow-ups.
Conclusion: PCP is rare in B-cell precursor ALL patients receiving blinatumomab therapy but manifests with early onset and rapid disease progression. Despite prophylaxis, PCP infection cannot be ignored during blinatumomab therapy. Therefore, heightened attention is warranted when using blinatumomab therapy.
期刊介绍:
This journal publishes original research articles and state-of-the-art reviews on all aspects of antimicrobial and antitumor chemotherapy. The results of experimental and clinical investigations into the microbiological and pharmacologic properties of antibacterial, antiviral and antitumor compounds are major topics of publication. Papers selected for the journal offer data concerning the efficacy, toxicology, and interactions of new drugs in single or combined applications. Studies designed to determine the pharmacokinetic and pharmacodynamics properties of similar preparations and comparing their efficacy are also included. Special emphasis is given to the development of drug-resistance, an increasing problem worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


