Anna Jansana, Aviane Auguste, Marina Kvaskoff, Agnès Fournier, Emma Fontvieille, Laia Peruchet-Noray, Carine Biessy, Reynalda Cordova, Kristina Elin Nielsen Petersen, Anne Tjønneland, Verena Katzke, Rudolf Kaaks, Fulvio Ricceri, Salvatore Panico, Paolo Contiero, Maria-Jose Sánchez, Jesus Castilla, Marta Crous-Bou, Alicia Heath, Elom Kouassivi Aglago, Elisabete Weiderpass, Marc James Gunter, Pietro Ferrari, Elio Riboli, Vivian Viallon, Heinz Freisling
{"title":"原有心脏代谢疾病对诊断时转移性癌症分期的影响:一项前瞻性多国队列研究。","authors":"Anna Jansana, Aviane Auguste, Marina Kvaskoff, Agnès Fournier, Emma Fontvieille, Laia Peruchet-Noray, Carine Biessy, Reynalda Cordova, Kristina Elin Nielsen Petersen, Anne Tjønneland, Verena Katzke, Rudolf Kaaks, Fulvio Ricceri, Salvatore Panico, Paolo Contiero, Maria-Jose Sánchez, Jesus Castilla, Marta Crous-Bou, Alicia Heath, Elom Kouassivi Aglago, Elisabete Weiderpass, Marc James Gunter, Pietro Ferrari, Elio Riboli, Vivian Viallon, Heinz Freisling","doi":"10.1002/cac2.12526","DOIUrl":null,"url":null,"abstract":"<p>Owing to shared risk factors between cardiometabolic diseases (CMDs) and cancer, coupled with population aging, the lifetime risk of an individual developing cancer after a CMD is increasing. Furthermore, biological mechanisms such as insulin resistance or inflammation may not only predispose individuals with CMD to an elevated risk of certain types of cancer but also to a diagnosis of cancer at an advanced stage [<span>1, 2</span>].</p><p>Cancer stage at diagnosis strongly correlates with cancer survival rates and impacts treatment decisions. Early cancer detection is key to improving cancer outcomes, especially for cancers with poor prognosis. Factors associated with a higher risk of an advanced-stage diagnosis may differ from those associated with cancer incidence. Previous studies support an association between advanced-stage cancer at diagnosis and certain patient characteristics, such as higher body mass index (BMI), older age, smoking, comorbidities, and cancer type. Studies examining the influence of comorbidities on cancer stage at diagnosis have suggested that a CMD requiring regular medical follow-up is associated with earlier cancer detection [<span>3, 4</span>]. However, studies have also suggested that overall participation rates in cancer screening programs may be lower among individuals with type 2 diabetes (T2D) or cardiovascular diseases (CVD), which may lead to later cancer detection and a more advanced stage at diagnosis [<span>5</span>].</p><p>A better understanding of how CMDs prior to cancer are associated with stage at cancer diagnosis may inform cancer screening recommendations. This study aimed to investigate whether having a pre-existing CMD is associated with late-stage cancer diagnosis and to identify potential modifiers of this association in the European Prospective Investigation into Cancer and Nutrition study (EPIC).</p><p>This multinational prospective cohort study included 11,945 individuals diagnosed with first primary cancer between 1992 and 2012. Of all the diagnosed cancers, 64.9% were localized, 35.1% were metastatic, 53.6% were diagnosed in women, and 4.8%, a, 7.1%, and 1.3% had a history of CVD, of T2D, and of both CVD and T2D, respectively (Supplementary Figure S1, Supplementary Table S1). In addition to overall cancer, breast and colorectal cancers (38.1% of all cancers) were also investigated separately because of the well-established population-based cancer screening programs for these two cancers at the time of cancer diagnosis in the countries included in this study (i.e., Denmark, Germany, Italy, Spain, Sweden, and the UK). Detailed methods are described in Supplementary Materials.</p><p>We found that the adjusted odds ratios (ORs) of developing metastatic cancer (vs. localized) comparing individuals with pre-existing CVD, T2D or both to those without a CMD prior to cancer were 0.92 (95% confidence interval [CI] = 0.65-1.01), 1.04 (95% CI = 0.83-1.18) and 1.06 (95% CI = 0.60-1.36), respectively (Figure 1). Among cancer patients diagnosed with cancers other than breast or colorectum (i.e., “other cancers”), the OR for the association between pre-existing T2D and metastatic cancer diagnosis was 1.12 (95% CI = 0.85-1.49), whereas no association was observed for pre-existing CVD (OR = 0.98; 95% CI = 0.67-1.15). Not adjusting for cancer site led to a substantial difference in estimates for other cancers, whereby individuals with pre-existing T2D as compared to individuals without a CMD had a higher risk of a late-stage diagnosis (OR = 1.26; 95% CI = 1.04-1.55) (Supplementary Figure S2). Among patients with breast and colorectal cancers, pre-existing CVD, as compared to no CMD, was almost inversely associated with a metastatic cancer diagnosis (OR of metastatic cancer = 0.71; 95% CI = 0.48-1.07). Point estimates were similar for both breast and colorectal cancer-specific analysis (Figure 1).</p><p>A few differences in associations across pre-defined subgroups of the study population were observed. There was suggestive evidence that associations between CMD status and metastatic cancer diagnosis were more pronounced among the younger age group (30-65 years) compared to the older age group (≥ 66 years), both for breast and colorectal cancers (<i>P</i> = 0.008) and other cancers (<i>p</i>-interaction = 0.017). There was evidence for effect modification by smoking status for other cancers (<i>P</i> = 0.032). The positive association between T2D status and diagnosis of metastatic other cancers was stronger in never smokers (OR: 1.60; 95% CI 1.04-2.46) than in former/current smokers (OR: 1.21; 95% CI 0.96-1.54) (Supplementary Table S2). This could be explained by fewer surveillance opportunities for non-smokers compared to individuals who smoked [<span>6</span>].</p><p>Our study supports prior findings as reviewed by Boakye et al. [<span>7</span>], who reported that T2D was associated with a higher risk of late-stage diagnosis of all cancers combined, whereas myocardial infarction was inversely associated with a late-stage diagnosis. We also found important differences. First, the positive association between T2D and a late-stage diagnosis was restricted to cancers not covered by population-based screening programs. Furthermore, the observation that this association became stronger when not adjusting for cancer type suggests that adults with T2D have a higher risk of cancers that are more frequently diagnosed at metastatic stages. In contrast, the suggestive inverse association between CVD and a late-stage diagnosis was restricted to cancers with population-wide screening (i.e., breast and colorectal cancers in our study). Second, there was evidence for effect modification of these associations by age group and smoking status.</p><p>Mechanisms by which chronic diseases might interfere with a timely cancer diagnosis include competing demands, whereby a chronic disease with high care complexity may delay cancer diagnosis due to masking of or undetected symptoms. It has also been suggested that patients with a high frequency of visits to health services may be reluctant to undergo additional diagnostic tests by health professionals. Lastly, biological mechanisms affecting cancer progression, such as hyperinsulinemia, inflammation pathways or shared risk factors, may explain the relation between CMDs and late-stage cancer diagnosis [<span>1, 8</span>]. In contrast, mechanisms facilitating a timely cancer diagnosis include more frequent contact with healthcare services, thereby providing surveillance opportunities to discuss possible cancer symptoms and second, some treatments for chronic diseases may reduce the risk of progression to metastatic disease (e.g., aspirin and colorectal cancer) [<span>1, 9</span>].</p><p>Studies investigating specific comorbidities and stage at diagnosis are scarce for cancers other than breast and colorectal cancers [<span>7</span>]. Nevertheless, patients with newly diagnosed T2D or hyperinsulinemia have been recommended for pancreatic and liver cancer screening since the presence of pre-existing disease may mask other diseases and thus lead to late cancer presentation [<span>10</span>]. Such recommendations for screening are supported by our findings. For other cancer sites, such as respiratory or hematologic cancers, studies have not shown an impact of pre-existing CMD on cancer stage at diagnosis [<span>7</span>].</p><p>Strengths of our study include the use of validated CMD diagnoses, including data on the duration of the comorbidity. Furthermore, the availability of data on a wide range of dietary and lifestyle variables enabled comprehensive adjustment for confounders. Limitations of our study include the lack of data on CVD/T2D management, lack of repeated assessment of confounders (e.g., lifestyle factors), and the limited sample size, which did not allow analyses for less frequent cancers (Supplementary Table S3). Study participants were invited from the general adult population in most study centers apart from some centers in Italy and Spain (blood donors), Utrecht and Florence (women invited for a local population-based breast cancer screening program), and Oxford (half of the recruited participants did not eat meat). Generalizing observed results beyond our study population should therefore be done with caution.</p><p>In this prospective multinational cohort study, cancer patients with pre-existing CVD, T2D or both were overall not more likely to be diagnosed with late-stage cancer. Further studies are needed to confirm the suggestive positive association between T2D vs. no CMD and late-stage cancer among patients with cancers not included in population-based screening.</p><p>Conceived and designed the study: Heinz Freisling. Analyzed the data: Anna Jansana. Supported data analysis: Carine Biessy, Vivian Viallon. Wrote the manuscript: Anna Jansana, Heinz Freisling. Has primary responsibility for the final content of the manuscript: Heinz Freisling. Critically reviewed the manuscript for important intellectual content and approved the final version: Anna Jansana, Aviane Auguste, Marina Kvaskoff, Carine Biessy, Agnès Fournier, Emma Fontvieille, Laia Peruchet-Noray, Reynalda Cordova, Kristina Elin Nielsen Petersen, Anne Tjønneland, Verena Katzke, Rudolf Kaaks, Fulvio Riccieri, Salvatore Panico, Paolo Contiero, Maria-Jose Sánchez, Jesus Castilla, Marta Crous-Bou, Alicia Heath, Elom Kouassivi Aglago, Elisabete Weiderpass, Marc James Gunter, Pietro Ferrari, Elio Riboli, Vivian Viallon, Heinz Freisling.</p><p>The authors declare that they have no competing interests.</p><p>This study was funded by the French National Cancer Institute (INCA_N°2018-123) and supported by Cancérôpole Ile-de-France (N°2018-1-PL SHS-06-CIRC-1). The coordination of EPIC is financially supported by the International Agency for Research on Cancer (IARC) and also by the Department of Epidemiology and Biostatistics, School of Public Health, Imperial College London, which has additional infrastructure support provided by the NIHR Imperial Biomedical Research Centre (BRC). The national cohorts are supported by: Danish Cancer Society (Denmark); Ligue Contre le Cancer, Institut Gustave Roussy, Mutuelle Générale de l'Education Nationale, Institut National de la Santé et de la Recherche Médicale (INSERM) (France); German Cancer Aid, German Cancer Research Center (DKFZ), German Institute of Human Nutrition Potsdam-Rehbruecke (DIfE), Federal Ministry of Education and Research (BMBF) (Germany); Associazione Italiana per la Ricerca sul Cancro-AIRC-Italy, Compagnia di SanPaolo and National Research Council (Italy); Dutch Ministry of Public Health, Welfare and Sports (VWS), Netherlands Cancer Registry (NKR), LK Research Funds, Dutch Prevention Funds, Dutch ZON (Zorg Onderzoek Nederland), World Cancer Research Fund (WCRF), Statistics Netherlands (The Netherlands); Health Research Fund (FIS) - Instituto de Salud Carlos III (ISCIII), Regional Governments of Andalucía, Asturias, Basque Country, Murcia and Navarra, and the Catalan Institute of Oncology - ICO (Spain); Swedish Cancer Society, Swedish Research Council and County Councils of Skåne and Västerbotten (Sweden); Cancer Research UK (14136 to EPIC-Norfolk; C8221/A29017 to EPIC-Oxford), Medical Research Council (1000143 to EPIC-Norfolk; MR/M012190/1 to EPIC-Oxford) (United Kingdom).</p><p>Ethical approval for the European Prospective Investigation into Cancer and Nutrition (EPIC) study was obtained from the International Agency for Research on Cancer and the ethical review boards of the participating institutes (permit number: IEC-10-07-2017). All participants provided written informed consent.</p><p>Not applicable.</p><p>Where authors are identified as personnel of the International Agency for Research on Cancer/ World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/ World Health Organization.</p>","PeriodicalId":9495,"journal":{"name":"Cancer Communications","volume":"44 5","pages":"593-597"},"PeriodicalIF":20.1000,"publicationDate":"2024-03-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12526","citationCount":"0","resultStr":"{\"title\":\"Impact of pre-existing cardiometabolic diseases on metastatic cancer stage at diagnosis: a prospective multinational cohort study\",\"authors\":\"Anna Jansana, Aviane Auguste, Marina Kvaskoff, Agnès Fournier, Emma Fontvieille, Laia Peruchet-Noray, Carine Biessy, Reynalda Cordova, Kristina Elin Nielsen Petersen, Anne Tjønneland, Verena Katzke, Rudolf Kaaks, Fulvio Ricceri, Salvatore Panico, Paolo Contiero, Maria-Jose Sánchez, Jesus Castilla, Marta Crous-Bou, Alicia Heath, Elom Kouassivi Aglago, Elisabete Weiderpass, Marc James Gunter, Pietro Ferrari, Elio Riboli, Vivian Viallon, Heinz Freisling\",\"doi\":\"10.1002/cac2.12526\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Owing to shared risk factors between cardiometabolic diseases (CMDs) and cancer, coupled with population aging, the lifetime risk of an individual developing cancer after a CMD is increasing. Furthermore, biological mechanisms such as insulin resistance or inflammation may not only predispose individuals with CMD to an elevated risk of certain types of cancer but also to a diagnosis of cancer at an advanced stage [<span>1, 2</span>].</p><p>Cancer stage at diagnosis strongly correlates with cancer survival rates and impacts treatment decisions. Early cancer detection is key to improving cancer outcomes, especially for cancers with poor prognosis. Factors associated with a higher risk of an advanced-stage diagnosis may differ from those associated with cancer incidence. Previous studies support an association between advanced-stage cancer at diagnosis and certain patient characteristics, such as higher body mass index (BMI), older age, smoking, comorbidities, and cancer type. Studies examining the influence of comorbidities on cancer stage at diagnosis have suggested that a CMD requiring regular medical follow-up is associated with earlier cancer detection [<span>3, 4</span>]. However, studies have also suggested that overall participation rates in cancer screening programs may be lower among individuals with type 2 diabetes (T2D) or cardiovascular diseases (CVD), which may lead to later cancer detection and a more advanced stage at diagnosis [<span>5</span>].</p><p>A better understanding of how CMDs prior to cancer are associated with stage at cancer diagnosis may inform cancer screening recommendations. This study aimed to investigate whether having a pre-existing CMD is associated with late-stage cancer diagnosis and to identify potential modifiers of this association in the European Prospective Investigation into Cancer and Nutrition study (EPIC).</p><p>This multinational prospective cohort study included 11,945 individuals diagnosed with first primary cancer between 1992 and 2012. Of all the diagnosed cancers, 64.9% were localized, 35.1% were metastatic, 53.6% were diagnosed in women, and 4.8%, a, 7.1%, and 1.3% had a history of CVD, of T2D, and of both CVD and T2D, respectively (Supplementary Figure S1, Supplementary Table S1). In addition to overall cancer, breast and colorectal cancers (38.1% of all cancers) were also investigated separately because of the well-established population-based cancer screening programs for these two cancers at the time of cancer diagnosis in the countries included in this study (i.e., Denmark, Germany, Italy, Spain, Sweden, and the UK). Detailed methods are described in Supplementary Materials.</p><p>We found that the adjusted odds ratios (ORs) of developing metastatic cancer (vs. localized) comparing individuals with pre-existing CVD, T2D or both to those without a CMD prior to cancer were 0.92 (95% confidence interval [CI] = 0.65-1.01), 1.04 (95% CI = 0.83-1.18) and 1.06 (95% CI = 0.60-1.36), respectively (Figure 1). Among cancer patients diagnosed with cancers other than breast or colorectum (i.e., “other cancers”), the OR for the association between pre-existing T2D and metastatic cancer diagnosis was 1.12 (95% CI = 0.85-1.49), whereas no association was observed for pre-existing CVD (OR = 0.98; 95% CI = 0.67-1.15). Not adjusting for cancer site led to a substantial difference in estimates for other cancers, whereby individuals with pre-existing T2D as compared to individuals without a CMD had a higher risk of a late-stage diagnosis (OR = 1.26; 95% CI = 1.04-1.55) (Supplementary Figure S2). Among patients with breast and colorectal cancers, pre-existing CVD, as compared to no CMD, was almost inversely associated with a metastatic cancer diagnosis (OR of metastatic cancer = 0.71; 95% CI = 0.48-1.07). Point estimates were similar for both breast and colorectal cancer-specific analysis (Figure 1).</p><p>A few differences in associations across pre-defined subgroups of the study population were observed. There was suggestive evidence that associations between CMD status and metastatic cancer diagnosis were more pronounced among the younger age group (30-65 years) compared to the older age group (≥ 66 years), both for breast and colorectal cancers (<i>P</i> = 0.008) and other cancers (<i>p</i>-interaction = 0.017). There was evidence for effect modification by smoking status for other cancers (<i>P</i> = 0.032). The positive association between T2D status and diagnosis of metastatic other cancers was stronger in never smokers (OR: 1.60; 95% CI 1.04-2.46) than in former/current smokers (OR: 1.21; 95% CI 0.96-1.54) (Supplementary Table S2). This could be explained by fewer surveillance opportunities for non-smokers compared to individuals who smoked [<span>6</span>].</p><p>Our study supports prior findings as reviewed by Boakye et al. [<span>7</span>], who reported that T2D was associated with a higher risk of late-stage diagnosis of all cancers combined, whereas myocardial infarction was inversely associated with a late-stage diagnosis. We also found important differences. First, the positive association between T2D and a late-stage diagnosis was restricted to cancers not covered by population-based screening programs. Furthermore, the observation that this association became stronger when not adjusting for cancer type suggests that adults with T2D have a higher risk of cancers that are more frequently diagnosed at metastatic stages. In contrast, the suggestive inverse association between CVD and a late-stage diagnosis was restricted to cancers with population-wide screening (i.e., breast and colorectal cancers in our study). Second, there was evidence for effect modification of these associations by age group and smoking status.</p><p>Mechanisms by which chronic diseases might interfere with a timely cancer diagnosis include competing demands, whereby a chronic disease with high care complexity may delay cancer diagnosis due to masking of or undetected symptoms. It has also been suggested that patients with a high frequency of visits to health services may be reluctant to undergo additional diagnostic tests by health professionals. Lastly, biological mechanisms affecting cancer progression, such as hyperinsulinemia, inflammation pathways or shared risk factors, may explain the relation between CMDs and late-stage cancer diagnosis [<span>1, 8</span>]. In contrast, mechanisms facilitating a timely cancer diagnosis include more frequent contact with healthcare services, thereby providing surveillance opportunities to discuss possible cancer symptoms and second, some treatments for chronic diseases may reduce the risk of progression to metastatic disease (e.g., aspirin and colorectal cancer) [<span>1, 9</span>].</p><p>Studies investigating specific comorbidities and stage at diagnosis are scarce for cancers other than breast and colorectal cancers [<span>7</span>]. Nevertheless, patients with newly diagnosed T2D or hyperinsulinemia have been recommended for pancreatic and liver cancer screening since the presence of pre-existing disease may mask other diseases and thus lead to late cancer presentation [<span>10</span>]. Such recommendations for screening are supported by our findings. For other cancer sites, such as respiratory or hematologic cancers, studies have not shown an impact of pre-existing CMD on cancer stage at diagnosis [<span>7</span>].</p><p>Strengths of our study include the use of validated CMD diagnoses, including data on the duration of the comorbidity. Furthermore, the availability of data on a wide range of dietary and lifestyle variables enabled comprehensive adjustment for confounders. Limitations of our study include the lack of data on CVD/T2D management, lack of repeated assessment of confounders (e.g., lifestyle factors), and the limited sample size, which did not allow analyses for less frequent cancers (Supplementary Table S3). Study participants were invited from the general adult population in most study centers apart from some centers in Italy and Spain (blood donors), Utrecht and Florence (women invited for a local population-based breast cancer screening program), and Oxford (half of the recruited participants did not eat meat). Generalizing observed results beyond our study population should therefore be done with caution.</p><p>In this prospective multinational cohort study, cancer patients with pre-existing CVD, T2D or both were overall not more likely to be diagnosed with late-stage cancer. Further studies are needed to confirm the suggestive positive association between T2D vs. no CMD and late-stage cancer among patients with cancers not included in population-based screening.</p><p>Conceived and designed the study: Heinz Freisling. Analyzed the data: Anna Jansana. Supported data analysis: Carine Biessy, Vivian Viallon. Wrote the manuscript: Anna Jansana, Heinz Freisling. Has primary responsibility for the final content of the manuscript: Heinz Freisling. Critically reviewed the manuscript for important intellectual content and approved the final version: Anna Jansana, Aviane Auguste, Marina Kvaskoff, Carine Biessy, Agnès Fournier, Emma Fontvieille, Laia Peruchet-Noray, Reynalda Cordova, Kristina Elin Nielsen Petersen, Anne Tjønneland, Verena Katzke, Rudolf Kaaks, Fulvio Riccieri, Salvatore Panico, Paolo Contiero, Maria-Jose Sánchez, Jesus Castilla, Marta Crous-Bou, Alicia Heath, Elom Kouassivi Aglago, Elisabete Weiderpass, Marc James Gunter, Pietro Ferrari, Elio Riboli, Vivian Viallon, Heinz Freisling.</p><p>The authors declare that they have no competing interests.</p><p>This study was funded by the French National Cancer Institute (INCA_N°2018-123) and supported by Cancérôpole Ile-de-France (N°2018-1-PL SHS-06-CIRC-1). The coordination of EPIC is financially supported by the International Agency for Research on Cancer (IARC) and also by the Department of Epidemiology and Biostatistics, School of Public Health, Imperial College London, which has additional infrastructure support provided by the NIHR Imperial Biomedical Research Centre (BRC). The national cohorts are supported by: Danish Cancer Society (Denmark); Ligue Contre le Cancer, Institut Gustave Roussy, Mutuelle Générale de l'Education Nationale, Institut National de la Santé et de la Recherche Médicale (INSERM) (France); German Cancer Aid, German Cancer Research Center (DKFZ), German Institute of Human Nutrition Potsdam-Rehbruecke (DIfE), Federal Ministry of Education and Research (BMBF) (Germany); Associazione Italiana per la Ricerca sul Cancro-AIRC-Italy, Compagnia di SanPaolo and National Research Council (Italy); Dutch Ministry of Public Health, Welfare and Sports (VWS), Netherlands Cancer Registry (NKR), LK Research Funds, Dutch Prevention Funds, Dutch ZON (Zorg Onderzoek Nederland), World Cancer Research Fund (WCRF), Statistics Netherlands (The Netherlands); Health Research Fund (FIS) - Instituto de Salud Carlos III (ISCIII), Regional Governments of Andalucía, Asturias, Basque Country, Murcia and Navarra, and the Catalan Institute of Oncology - ICO (Spain); Swedish Cancer Society, Swedish Research Council and County Councils of Skåne and Västerbotten (Sweden); Cancer Research UK (14136 to EPIC-Norfolk; C8221/A29017 to EPIC-Oxford), Medical Research Council (1000143 to EPIC-Norfolk; MR/M012190/1 to EPIC-Oxford) (United Kingdom).</p><p>Ethical approval for the European Prospective Investigation into Cancer and Nutrition (EPIC) study was obtained from the International Agency for Research on Cancer and the ethical review boards of the participating institutes (permit number: IEC-10-07-2017). All participants provided written informed consent.</p><p>Not applicable.</p><p>Where authors are identified as personnel of the International Agency for Research on Cancer/ World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/ World Health Organization.</p>\",\"PeriodicalId\":9495,\"journal\":{\"name\":\"Cancer Communications\",\"volume\":\"44 5\",\"pages\":\"593-597\"},\"PeriodicalIF\":20.1000,\"publicationDate\":\"2024-03-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12526\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Communications\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12526\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Communications","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12526","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
Impact of pre-existing cardiometabolic diseases on metastatic cancer stage at diagnosis: a prospective multinational cohort study
Owing to shared risk factors between cardiometabolic diseases (CMDs) and cancer, coupled with population aging, the lifetime risk of an individual developing cancer after a CMD is increasing. Furthermore, biological mechanisms such as insulin resistance or inflammation may not only predispose individuals with CMD to an elevated risk of certain types of cancer but also to a diagnosis of cancer at an advanced stage [1, 2].
Cancer stage at diagnosis strongly correlates with cancer survival rates and impacts treatment decisions. Early cancer detection is key to improving cancer outcomes, especially for cancers with poor prognosis. Factors associated with a higher risk of an advanced-stage diagnosis may differ from those associated with cancer incidence. Previous studies support an association between advanced-stage cancer at diagnosis and certain patient characteristics, such as higher body mass index (BMI), older age, smoking, comorbidities, and cancer type. Studies examining the influence of comorbidities on cancer stage at diagnosis have suggested that a CMD requiring regular medical follow-up is associated with earlier cancer detection [3, 4]. However, studies have also suggested that overall participation rates in cancer screening programs may be lower among individuals with type 2 diabetes (T2D) or cardiovascular diseases (CVD), which may lead to later cancer detection and a more advanced stage at diagnosis [5].
A better understanding of how CMDs prior to cancer are associated with stage at cancer diagnosis may inform cancer screening recommendations. This study aimed to investigate whether having a pre-existing CMD is associated with late-stage cancer diagnosis and to identify potential modifiers of this association in the European Prospective Investigation into Cancer and Nutrition study (EPIC).
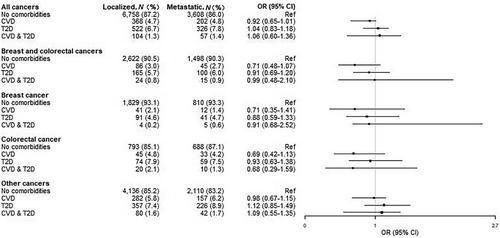
This multinational prospective cohort study included 11,945 individuals diagnosed with first primary cancer between 1992 and 2012. Of all the diagnosed cancers, 64.9% were localized, 35.1% were metastatic, 53.6% were diagnosed in women, and 4.8%, a, 7.1%, and 1.3% had a history of CVD, of T2D, and of both CVD and T2D, respectively (Supplementary Figure S1, Supplementary Table S1). In addition to overall cancer, breast and colorectal cancers (38.1% of all cancers) were also investigated separately because of the well-established population-based cancer screening programs for these two cancers at the time of cancer diagnosis in the countries included in this study (i.e., Denmark, Germany, Italy, Spain, Sweden, and the UK). Detailed methods are described in Supplementary Materials.
We found that the adjusted odds ratios (ORs) of developing metastatic cancer (vs. localized) comparing individuals with pre-existing CVD, T2D or both to those without a CMD prior to cancer were 0.92 (95% confidence interval [CI] = 0.65-1.01), 1.04 (95% CI = 0.83-1.18) and 1.06 (95% CI = 0.60-1.36), respectively (Figure 1). Among cancer patients diagnosed with cancers other than breast or colorectum (i.e., “other cancers”), the OR for the association between pre-existing T2D and metastatic cancer diagnosis was 1.12 (95% CI = 0.85-1.49), whereas no association was observed for pre-existing CVD (OR = 0.98; 95% CI = 0.67-1.15). Not adjusting for cancer site led to a substantial difference in estimates for other cancers, whereby individuals with pre-existing T2D as compared to individuals without a CMD had a higher risk of a late-stage diagnosis (OR = 1.26; 95% CI = 1.04-1.55) (Supplementary Figure S2). Among patients with breast and colorectal cancers, pre-existing CVD, as compared to no CMD, was almost inversely associated with a metastatic cancer diagnosis (OR of metastatic cancer = 0.71; 95% CI = 0.48-1.07). Point estimates were similar for both breast and colorectal cancer-specific analysis (Figure 1).
A few differences in associations across pre-defined subgroups of the study population were observed. There was suggestive evidence that associations between CMD status and metastatic cancer diagnosis were more pronounced among the younger age group (30-65 years) compared to the older age group (≥ 66 years), both for breast and colorectal cancers (P = 0.008) and other cancers (p-interaction = 0.017). There was evidence for effect modification by smoking status for other cancers (P = 0.032). The positive association between T2D status and diagnosis of metastatic other cancers was stronger in never smokers (OR: 1.60; 95% CI 1.04-2.46) than in former/current smokers (OR: 1.21; 95% CI 0.96-1.54) (Supplementary Table S2). This could be explained by fewer surveillance opportunities for non-smokers compared to individuals who smoked [6].
Our study supports prior findings as reviewed by Boakye et al. [7], who reported that T2D was associated with a higher risk of late-stage diagnosis of all cancers combined, whereas myocardial infarction was inversely associated with a late-stage diagnosis. We also found important differences. First, the positive association between T2D and a late-stage diagnosis was restricted to cancers not covered by population-based screening programs. Furthermore, the observation that this association became stronger when not adjusting for cancer type suggests that adults with T2D have a higher risk of cancers that are more frequently diagnosed at metastatic stages. In contrast, the suggestive inverse association between CVD and a late-stage diagnosis was restricted to cancers with population-wide screening (i.e., breast and colorectal cancers in our study). Second, there was evidence for effect modification of these associations by age group and smoking status.
Mechanisms by which chronic diseases might interfere with a timely cancer diagnosis include competing demands, whereby a chronic disease with high care complexity may delay cancer diagnosis due to masking of or undetected symptoms. It has also been suggested that patients with a high frequency of visits to health services may be reluctant to undergo additional diagnostic tests by health professionals. Lastly, biological mechanisms affecting cancer progression, such as hyperinsulinemia, inflammation pathways or shared risk factors, may explain the relation between CMDs and late-stage cancer diagnosis [1, 8]. In contrast, mechanisms facilitating a timely cancer diagnosis include more frequent contact with healthcare services, thereby providing surveillance opportunities to discuss possible cancer symptoms and second, some treatments for chronic diseases may reduce the risk of progression to metastatic disease (e.g., aspirin and colorectal cancer) [1, 9].
Studies investigating specific comorbidities and stage at diagnosis are scarce for cancers other than breast and colorectal cancers [7]. Nevertheless, patients with newly diagnosed T2D or hyperinsulinemia have been recommended for pancreatic and liver cancer screening since the presence of pre-existing disease may mask other diseases and thus lead to late cancer presentation [10]. Such recommendations for screening are supported by our findings. For other cancer sites, such as respiratory or hematologic cancers, studies have not shown an impact of pre-existing CMD on cancer stage at diagnosis [7].
Strengths of our study include the use of validated CMD diagnoses, including data on the duration of the comorbidity. Furthermore, the availability of data on a wide range of dietary and lifestyle variables enabled comprehensive adjustment for confounders. Limitations of our study include the lack of data on CVD/T2D management, lack of repeated assessment of confounders (e.g., lifestyle factors), and the limited sample size, which did not allow analyses for less frequent cancers (Supplementary Table S3). Study participants were invited from the general adult population in most study centers apart from some centers in Italy and Spain (blood donors), Utrecht and Florence (women invited for a local population-based breast cancer screening program), and Oxford (half of the recruited participants did not eat meat). Generalizing observed results beyond our study population should therefore be done with caution.
In this prospective multinational cohort study, cancer patients with pre-existing CVD, T2D or both were overall not more likely to be diagnosed with late-stage cancer. Further studies are needed to confirm the suggestive positive association between T2D vs. no CMD and late-stage cancer among patients with cancers not included in population-based screening.
Conceived and designed the study: Heinz Freisling. Analyzed the data: Anna Jansana. Supported data analysis: Carine Biessy, Vivian Viallon. Wrote the manuscript: Anna Jansana, Heinz Freisling. Has primary responsibility for the final content of the manuscript: Heinz Freisling. Critically reviewed the manuscript for important intellectual content and approved the final version: Anna Jansana, Aviane Auguste, Marina Kvaskoff, Carine Biessy, Agnès Fournier, Emma Fontvieille, Laia Peruchet-Noray, Reynalda Cordova, Kristina Elin Nielsen Petersen, Anne Tjønneland, Verena Katzke, Rudolf Kaaks, Fulvio Riccieri, Salvatore Panico, Paolo Contiero, Maria-Jose Sánchez, Jesus Castilla, Marta Crous-Bou, Alicia Heath, Elom Kouassivi Aglago, Elisabete Weiderpass, Marc James Gunter, Pietro Ferrari, Elio Riboli, Vivian Viallon, Heinz Freisling.
The authors declare that they have no competing interests.
This study was funded by the French National Cancer Institute (INCA_N°2018-123) and supported by Cancérôpole Ile-de-France (N°2018-1-PL SHS-06-CIRC-1). The coordination of EPIC is financially supported by the International Agency for Research on Cancer (IARC) and also by the Department of Epidemiology and Biostatistics, School of Public Health, Imperial College London, which has additional infrastructure support provided by the NIHR Imperial Biomedical Research Centre (BRC). The national cohorts are supported by: Danish Cancer Society (Denmark); Ligue Contre le Cancer, Institut Gustave Roussy, Mutuelle Générale de l'Education Nationale, Institut National de la Santé et de la Recherche Médicale (INSERM) (France); German Cancer Aid, German Cancer Research Center (DKFZ), German Institute of Human Nutrition Potsdam-Rehbruecke (DIfE), Federal Ministry of Education and Research (BMBF) (Germany); Associazione Italiana per la Ricerca sul Cancro-AIRC-Italy, Compagnia di SanPaolo and National Research Council (Italy); Dutch Ministry of Public Health, Welfare and Sports (VWS), Netherlands Cancer Registry (NKR), LK Research Funds, Dutch Prevention Funds, Dutch ZON (Zorg Onderzoek Nederland), World Cancer Research Fund (WCRF), Statistics Netherlands (The Netherlands); Health Research Fund (FIS) - Instituto de Salud Carlos III (ISCIII), Regional Governments of Andalucía, Asturias, Basque Country, Murcia and Navarra, and the Catalan Institute of Oncology - ICO (Spain); Swedish Cancer Society, Swedish Research Council and County Councils of Skåne and Västerbotten (Sweden); Cancer Research UK (14136 to EPIC-Norfolk; C8221/A29017 to EPIC-Oxford), Medical Research Council (1000143 to EPIC-Norfolk; MR/M012190/1 to EPIC-Oxford) (United Kingdom).
Ethical approval for the European Prospective Investigation into Cancer and Nutrition (EPIC) study was obtained from the International Agency for Research on Cancer and the ethical review boards of the participating institutes (permit number: IEC-10-07-2017). All participants provided written informed consent.
Not applicable.
Where authors are identified as personnel of the International Agency for Research on Cancer/ World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/ World Health Organization.
期刊介绍:
Cancer Communications is an open access, peer-reviewed online journal that encompasses basic, clinical, and translational cancer research. The journal welcomes submissions concerning clinical trials, epidemiology, molecular and cellular biology, and genetics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


