{"title":"正畸治疗中下颌臼齿远化的边界:系统回顾和荟萃分析。","authors":"Keyuan Liu, Guang Chu, Chengfei Zhang, Yanqi Yang","doi":"10.1111/ocr.12778","DOIUrl":null,"url":null,"abstract":"<p>To explore the mandibular retromolar space length (MRSL), initial root-inner cortex contact percentage (IRCCP), and the various factors that influence mandibular molar distalization. Searches were undertaken in PubMed, EMBASE, Web of Science, Cochrane Library, Scopus, and grey literature (Google Scholar and OpenGrey) for eligible cross-sectional observational studies measuring the MRSL and IRCCP in healthy adult patients. The risk of bias and evidence quality were evaluated using the Joanna Briggs Institute's checklist and GRADE framework. Thirteen studies involving 1169 patients were included for qualitative synthesis. Seven of these studies were eligible for quantitative analysis. Meta-analysis showed that the mean MRSL at the subfurcation-6 mm plane in Asian normodivergent cases was 3.78 mm (95% confidence interval [CI]: 2.81–4.35; <i>I</i><sup>2</sup> = 79.7%) for skeletal Class-I malocclusions, 3.02 mm (95% CI: 2.10–3.94; <i>I</i><sup>2</sup> = 62.5%) for Class-II, and 4.43 mm (95% CI: 3.14–5.73; <i>I</i><sup>2</sup> = 75.1%) for Class-III. The mean MRSL at the sub-cementoenamel junction (CEJ)-10 mm plane for Asian, Class-I, normodivergent cases was 3.28 mm (95% CI: 2.44–4.12; <i>I</i><sup>2</sup> = 68.9%). The mean IRCCP for Asian, Class-I, normodivergent cases was 27.2% (95% CI: 0.22–0.32; <i>I</i><sup>2</sup> = 0%). In Asian normodivergent cases, MRSL ranges from 3.28 to 4.43 mm with a 27.2% IRCCP for Class-I. Cone-beam computed tomography imaging is recommended for measuring the MRSL in the apex region particularly before molar distalization. Factors influencing MRSL and IRCCP include different races, skeletal patterns, facial types, and third-molar status.</p>","PeriodicalId":19652,"journal":{"name":"Orthodontics & Craniofacial Research","volume":"27 4","pages":"515-526"},"PeriodicalIF":2.4000,"publicationDate":"2024-03-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ocr.12778","citationCount":"0","resultStr":"{\"title\":\"Boundary of mandibular molar distalization in orthodontic treatment: A systematic review and meta-analysis\",\"authors\":\"Keyuan Liu, Guang Chu, Chengfei Zhang, Yanqi Yang\",\"doi\":\"10.1111/ocr.12778\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>To explore the mandibular retromolar space length (MRSL), initial root-inner cortex contact percentage (IRCCP), and the various factors that influence mandibular molar distalization. Searches were undertaken in PubMed, EMBASE, Web of Science, Cochrane Library, Scopus, and grey literature (Google Scholar and OpenGrey) for eligible cross-sectional observational studies measuring the MRSL and IRCCP in healthy adult patients. The risk of bias and evidence quality were evaluated using the Joanna Briggs Institute's checklist and GRADE framework. Thirteen studies involving 1169 patients were included for qualitative synthesis. Seven of these studies were eligible for quantitative analysis. Meta-analysis showed that the mean MRSL at the subfurcation-6 mm plane in Asian normodivergent cases was 3.78 mm (95% confidence interval [CI]: 2.81–4.35; <i>I</i><sup>2</sup> = 79.7%) for skeletal Class-I malocclusions, 3.02 mm (95% CI: 2.10–3.94; <i>I</i><sup>2</sup> = 62.5%) for Class-II, and 4.43 mm (95% CI: 3.14–5.73; <i>I</i><sup>2</sup> = 75.1%) for Class-III. The mean MRSL at the sub-cementoenamel junction (CEJ)-10 mm plane for Asian, Class-I, normodivergent cases was 3.28 mm (95% CI: 2.44–4.12; <i>I</i><sup>2</sup> = 68.9%). The mean IRCCP for Asian, Class-I, normodivergent cases was 27.2% (95% CI: 0.22–0.32; <i>I</i><sup>2</sup> = 0%). In Asian normodivergent cases, MRSL ranges from 3.28 to 4.43 mm with a 27.2% IRCCP for Class-I. Cone-beam computed tomography imaging is recommended for measuring the MRSL in the apex region particularly before molar distalization. Factors influencing MRSL and IRCCP include different races, skeletal patterns, facial types, and third-molar status.</p>\",\"PeriodicalId\":19652,\"journal\":{\"name\":\"Orthodontics & Craniofacial Research\",\"volume\":\"27 4\",\"pages\":\"515-526\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-03-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ocr.12778\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Orthodontics & Craniofacial Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ocr.12778\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"DENTISTRY, ORAL SURGERY & MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Orthodontics & Craniofacial Research","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ocr.12778","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
Boundary of mandibular molar distalization in orthodontic treatment: A systematic review and meta-analysis
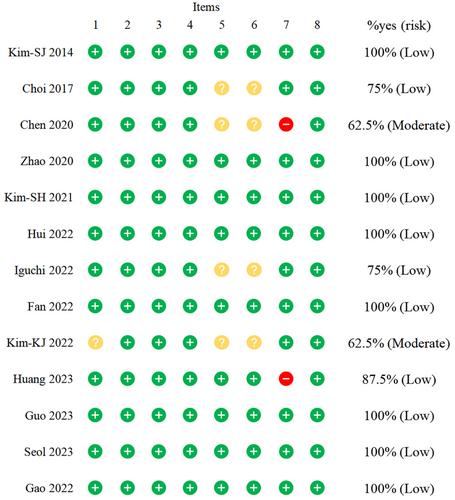
To explore the mandibular retromolar space length (MRSL), initial root-inner cortex contact percentage (IRCCP), and the various factors that influence mandibular molar distalization. Searches were undertaken in PubMed, EMBASE, Web of Science, Cochrane Library, Scopus, and grey literature (Google Scholar and OpenGrey) for eligible cross-sectional observational studies measuring the MRSL and IRCCP in healthy adult patients. The risk of bias and evidence quality were evaluated using the Joanna Briggs Institute's checklist and GRADE framework. Thirteen studies involving 1169 patients were included for qualitative synthesis. Seven of these studies were eligible for quantitative analysis. Meta-analysis showed that the mean MRSL at the subfurcation-6 mm plane in Asian normodivergent cases was 3.78 mm (95% confidence interval [CI]: 2.81–4.35; I2 = 79.7%) for skeletal Class-I malocclusions, 3.02 mm (95% CI: 2.10–3.94; I2 = 62.5%) for Class-II, and 4.43 mm (95% CI: 3.14–5.73; I2 = 75.1%) for Class-III. The mean MRSL at the sub-cementoenamel junction (CEJ)-10 mm plane for Asian, Class-I, normodivergent cases was 3.28 mm (95% CI: 2.44–4.12; I2 = 68.9%). The mean IRCCP for Asian, Class-I, normodivergent cases was 27.2% (95% CI: 0.22–0.32; I2 = 0%). In Asian normodivergent cases, MRSL ranges from 3.28 to 4.43 mm with a 27.2% IRCCP for Class-I. Cone-beam computed tomography imaging is recommended for measuring the MRSL in the apex region particularly before molar distalization. Factors influencing MRSL and IRCCP include different races, skeletal patterns, facial types, and third-molar status.
期刊介绍:
Orthodontics & Craniofacial Research - Genes, Growth and Development is published to serve its readers as an international forum for the presentation and critical discussion of issues pertinent to the advancement of the specialty of orthodontics and the evidence-based knowledge of craniofacial growth and development. This forum is based on scientifically supported information, but also includes minority and conflicting opinions.
The objective of the journal is to facilitate effective communication between the research community and practicing clinicians. Original papers of high scientific quality that report the findings of clinical trials, clinical epidemiology, and novel therapeutic or diagnostic approaches are appropriate submissions. Similarly, we welcome papers in genetics, developmental biology, syndromology, surgery, speech and hearing, and other biomedical disciplines related to clinical orthodontics and normal and abnormal craniofacial growth and development. In addition to original and basic research, the journal publishes concise reviews, case reports of substantial value, invited essays, letters, and announcements.
The journal is published quarterly. The review of submitted papers will be coordinated by the editor and members of the editorial board. It is policy to review manuscripts within 3 to 4 weeks of receipt and to publish within 3 to 6 months of acceptance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


