Michael G Taylor, Jeanette R Bauchat, Laura L Sorabella, Jonathan P Wanderer, Xiaoke Feng, Matthew S Shotwell, Holly B Ende
{"title":"一项回顾性队列研究发现,在长期服用丁丙诺啡的产妇中,神经阻滞性克洛尼定与降低剖宫产后阿片类药物消耗量或疼痛评分无关。","authors":"Michael G Taylor, Jeanette R Bauchat, Laura L Sorabella, Jonathan P Wanderer, Xiaoke Feng, Matthew S Shotwell, Holly B Ende","doi":"10.1007/s00540-024-03314-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Adequate post-cesarean delivery analgesia can be difficult to achieve for women diagnosed with opioid use disorder receiving buprenorphine. We sought to determine if neuraxial clonidine administration is associated with decreased opioid consumption and pain scores following cesarean delivery in women receiving chronic buprenorphine therapy.</p><p><strong>Methods: </strong>This was a retrospective cohort study at a tertiary care teaching hospital of women undergoing cesarean delivery with or without neuraxial clonidine administration while receiving chronic buprenorphine. The primary outcome was opioid consumption (in morphine milligram equivalents) 0-6 h following cesarean delivery. Secondary outcomes included opioid consumption 0-24 h post-cesarean, median postoperative pain scores 0-24 h, and rates of intraoperative anesthetic supplementation. Multivariable analysis evaluating the adjusted effects of neuraxial clonidine on outcomes was conducted using linear regression, proportional odds model, and logistic regression separately.</p><p><strong>Results: </strong>196 women met inclusion criteria, of which 145 (74%) received neuraxial clonidine while 51 (26%) did not. In univariate analysis, there was no significant difference in opioid consumption 0-6 h post-cesarean delivery between the clonidine (8 [IQR 0, 15]) and control (1 [IQR 0, 8]) groups (P = 0.14). After adjusting for potential confounders, there remained no significant association with neuraxial clonidine administration 0-6 h (Difference in means 2.77, 95% CI [- 0.89 to 6.44], P = 0.14) or 0-24 h (Difference in means 8.56, 95% CI [- 16.99 to 34.11], P = 0.51).</p><p><strong>Conclusion: </strong>In parturients receiving chronic buprenorphine therapy at the time of cesarean delivery, neuraxial clonidine administration was not associated with decreased postoperative opioid consumption, median pain scores, or the need for intraoperative supplementation.</p>","PeriodicalId":14997,"journal":{"name":"Journal of Anesthesia","volume":null,"pages":null},"PeriodicalIF":2.8000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Neuraxial clonidine is not associated with lower post-cesarean opioid consumption or pain scores in parturients on chronic buprenorphine therapy: a retrospective cohort study.\",\"authors\":\"Michael G Taylor, Jeanette R Bauchat, Laura L Sorabella, Jonathan P Wanderer, Xiaoke Feng, Matthew S Shotwell, Holly B Ende\",\"doi\":\"10.1007/s00540-024-03314-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Adequate post-cesarean delivery analgesia can be difficult to achieve for women diagnosed with opioid use disorder receiving buprenorphine. We sought to determine if neuraxial clonidine administration is associated with decreased opioid consumption and pain scores following cesarean delivery in women receiving chronic buprenorphine therapy.</p><p><strong>Methods: </strong>This was a retrospective cohort study at a tertiary care teaching hospital of women undergoing cesarean delivery with or without neuraxial clonidine administration while receiving chronic buprenorphine. The primary outcome was opioid consumption (in morphine milligram equivalents) 0-6 h following cesarean delivery. Secondary outcomes included opioid consumption 0-24 h post-cesarean, median postoperative pain scores 0-24 h, and rates of intraoperative anesthetic supplementation. Multivariable analysis evaluating the adjusted effects of neuraxial clonidine on outcomes was conducted using linear regression, proportional odds model, and logistic regression separately.</p><p><strong>Results: </strong>196 women met inclusion criteria, of which 145 (74%) received neuraxial clonidine while 51 (26%) did not. In univariate analysis, there was no significant difference in opioid consumption 0-6 h post-cesarean delivery between the clonidine (8 [IQR 0, 15]) and control (1 [IQR 0, 8]) groups (P = 0.14). After adjusting for potential confounders, there remained no significant association with neuraxial clonidine administration 0-6 h (Difference in means 2.77, 95% CI [- 0.89 to 6.44], P = 0.14) or 0-24 h (Difference in means 8.56, 95% CI [- 16.99 to 34.11], P = 0.51).</p><p><strong>Conclusion: </strong>In parturients receiving chronic buprenorphine therapy at the time of cesarean delivery, neuraxial clonidine administration was not associated with decreased postoperative opioid consumption, median pain scores, or the need for intraoperative supplementation.</p>\",\"PeriodicalId\":14997,\"journal\":{\"name\":\"Journal of Anesthesia\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Anesthesia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00540-024-03314-8\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Anesthesia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00540-024-03314-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:对于被诊断患有阿片类药物使用障碍并正在接受丁丙诺啡治疗的妇女来说,很难实现充分的剖腹产后镇痛。我们试图确定神经阻滞性克洛尼定用药是否与长期接受丁丙诺啡治疗的产妇剖宫产后阿片类药物用量减少和疼痛评分降低有关:这是一项回顾性队列研究,研究对象是一家三级医疗教学医院的剖宫产产妇,在接受或不接受神经阻滞性氯尼替胺治疗的同时,还在接受长期丁丙诺啡治疗。主要结果是剖宫产后 0-6 h 的阿片类药物消耗量(以吗啡毫克当量计)。次要结果包括剖宫产后0-24小时的阿片类药物消耗量、0-24小时的术后疼痛评分中位数以及术中麻醉剂补充率。采用线性回归、比例几率模型和逻辑回归分别进行了多变量分析,以评估神经阻滞性氯尼替胺对结果的调整效应:196名妇女符合纳入标准,其中145人(74%)接受了神经阻滞性氯尼替胺治疗,51人(26%)未接受治疗。在单变量分析中,克洛尼定组(8 [IQR 0, 15])和对照组(1 [IQR 0, 8])在剖宫产后 0-6 h 的阿片类药物消耗量没有显著差异(P = 0.14)。在对潜在的混杂因素进行调整后,0-6 h(平均值差异为 2.77,95% CI [- 0.89 至 6.44],P = 0.14)或 0-24 h(平均值差异为 8.56,95% CI [- 16.99 至 34.11],P = 0.51)神经阻滞氯尼地定用药仍无明显关联:结论:在剖宫产时接受长期丁丙诺啡治疗的产妇中,神经阻滞氯尼丁与术后阿片类药物用量减少、中位疼痛评分降低或术中需要补充阿片类药物无关。
Neuraxial clonidine is not associated with lower post-cesarean opioid consumption or pain scores in parturients on chronic buprenorphine therapy: a retrospective cohort study.
Purpose: Adequate post-cesarean delivery analgesia can be difficult to achieve for women diagnosed with opioid use disorder receiving buprenorphine. We sought to determine if neuraxial clonidine administration is associated with decreased opioid consumption and pain scores following cesarean delivery in women receiving chronic buprenorphine therapy.
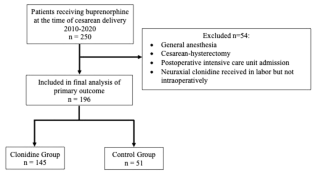
Methods: This was a retrospective cohort study at a tertiary care teaching hospital of women undergoing cesarean delivery with or without neuraxial clonidine administration while receiving chronic buprenorphine. The primary outcome was opioid consumption (in morphine milligram equivalents) 0-6 h following cesarean delivery. Secondary outcomes included opioid consumption 0-24 h post-cesarean, median postoperative pain scores 0-24 h, and rates of intraoperative anesthetic supplementation. Multivariable analysis evaluating the adjusted effects of neuraxial clonidine on outcomes was conducted using linear regression, proportional odds model, and logistic regression separately.
Results: 196 women met inclusion criteria, of which 145 (74%) received neuraxial clonidine while 51 (26%) did not. In univariate analysis, there was no significant difference in opioid consumption 0-6 h post-cesarean delivery between the clonidine (8 [IQR 0, 15]) and control (1 [IQR 0, 8]) groups (P = 0.14). After adjusting for potential confounders, there remained no significant association with neuraxial clonidine administration 0-6 h (Difference in means 2.77, 95% CI [- 0.89 to 6.44], P = 0.14) or 0-24 h (Difference in means 8.56, 95% CI [- 16.99 to 34.11], P = 0.51).
Conclusion: In parturients receiving chronic buprenorphine therapy at the time of cesarean delivery, neuraxial clonidine administration was not associated with decreased postoperative opioid consumption, median pain scores, or the need for intraoperative supplementation.
期刊介绍:
The Journal of Anesthesia is the official journal of the Japanese Society of Anesthesiologists. This journal publishes original articles, review articles, special articles, clinical reports, short communications, letters to the editor, and book and multimedia reviews. The editors welcome the submission of manuscripts devoted to anesthesia and related topics from any country of the world. Membership in the Society is not a prerequisite.
The Journal of Anesthesia (JA) welcomes case reports that show unique cases in perioperative medicine, intensive care, emergency medicine, and pain management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


