Christopher C. Paiz BS , Oluwafemi P. Owodunni MD, MPH , Evan N. Courville MD , Meic Schmidt MD, MBA , Robert Alunday MD , Christian A. Bowers
{"title":"虚弱程度可预测神经外科患者主要并发症后 30 天的死亡率:与改良虚弱指数-5 和患者年龄增加相比,风险分析指数具有更高的辨别能力","authors":"Christopher C. Paiz BS , Oluwafemi P. Owodunni MD, MPH , Evan N. Courville MD , Meic Schmidt MD, MBA , Robert Alunday MD , Christian A. Bowers","doi":"10.1016/j.wnsx.2024.100286","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Postoperative complications after cranial or spine surgery are prevalent, and frailty can be a key contributing patient factor. Therefore, we evaluated frailty’s impact on 30-day mortality. We compared the discrimination for risk analysis index (RAI), modified frailty index-5 (mFI-5) and increasing patient age for predicting 30-day mortality.</p></div><div><h3>Methods</h3><p>Patients with major complications following neurosurgery procedures between 2012- 2020 in the ACS-NSQIP database were included. We employed receiver operating characteristic (ROC) curve and examined discrimination thresholds for RAI, mFI-5, and increasing patient age for 30-day mortality. Independent relationships were examined using multivariable analysis.</p></div><div><h3>Results</h3><p>There were 19,096 patients included in the study and in the ROC analysis for 30-day mortality, RAI showed superior discriminant validity threshold C-statistic 0.655 (95% CI: 0.644-0.666), compared to mFI-5 C-statistic 0.570 (95% CI 0.559-0.581), and increasing patient age C-statistic 0.607 (95% CI 0.595-0.619). When the patient population was divided into subsets based on the procedures type (spinal, cranial or other), spine procedures had the highest discriminant validity threshold for RAI (Cstatistic 0.717). Furthermore, there was a frailty risk tier dose response relationship with 30-day mortalityy (p<0.001).</p></div><div><h3>Conclusion</h3><p>When a major complication arises after neurosurgical procedures, frail patients have a higher likelihood of dying within 30 days than their non-frail counterparts. The RAI demonstrated a higher discriminant validity threshold than mFI-5 and increasing patient age, making it a more clinically relevant tool for identifying and stratifying patients by frailty risk tiers. These findings highlight the importance of initiatives geared toward optimizing frail patients, to mitigate long-term disability.</p></div>","PeriodicalId":37134,"journal":{"name":"World Neurosurgery: X","volume":"23 ","pages":"Article 100286"},"PeriodicalIF":0.0000,"publicationDate":"2024-03-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2590139724000176/pdfft?md5=ca223edaf9bd16763d125a79b59422d3&pid=1-s2.0-S2590139724000176-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Frailty Predicts 30-day mortality following major complications in neurosurgery patients: The risk analysis index has superior discrimination compared to modified frailty index-5 and increasing patient age\",\"authors\":\"Christopher C. Paiz BS , Oluwafemi P. Owodunni MD, MPH , Evan N. Courville MD , Meic Schmidt MD, MBA , Robert Alunday MD , Christian A. Bowers\",\"doi\":\"10.1016/j.wnsx.2024.100286\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Postoperative complications after cranial or spine surgery are prevalent, and frailty can be a key contributing patient factor. Therefore, we evaluated frailty’s impact on 30-day mortality. We compared the discrimination for risk analysis index (RAI), modified frailty index-5 (mFI-5) and increasing patient age for predicting 30-day mortality.</p></div><div><h3>Methods</h3><p>Patients with major complications following neurosurgery procedures between 2012- 2020 in the ACS-NSQIP database were included. We employed receiver operating characteristic (ROC) curve and examined discrimination thresholds for RAI, mFI-5, and increasing patient age for 30-day mortality. Independent relationships were examined using multivariable analysis.</p></div><div><h3>Results</h3><p>There were 19,096 patients included in the study and in the ROC analysis for 30-day mortality, RAI showed superior discriminant validity threshold C-statistic 0.655 (95% CI: 0.644-0.666), compared to mFI-5 C-statistic 0.570 (95% CI 0.559-0.581), and increasing patient age C-statistic 0.607 (95% CI 0.595-0.619). When the patient population was divided into subsets based on the procedures type (spinal, cranial or other), spine procedures had the highest discriminant validity threshold for RAI (Cstatistic 0.717). Furthermore, there was a frailty risk tier dose response relationship with 30-day mortalityy (p<0.001).</p></div><div><h3>Conclusion</h3><p>When a major complication arises after neurosurgical procedures, frail patients have a higher likelihood of dying within 30 days than their non-frail counterparts. The RAI demonstrated a higher discriminant validity threshold than mFI-5 and increasing patient age, making it a more clinically relevant tool for identifying and stratifying patients by frailty risk tiers. These findings highlight the importance of initiatives geared toward optimizing frail patients, to mitigate long-term disability.</p></div>\",\"PeriodicalId\":37134,\"journal\":{\"name\":\"World Neurosurgery: X\",\"volume\":\"23 \",\"pages\":\"Article 100286\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-03-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2590139724000176/pdfft?md5=ca223edaf9bd16763d125a79b59422d3&pid=1-s2.0-S2590139724000176-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Neurosurgery: X\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590139724000176\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Neurosurgery: X","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590139724000176","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景 颅骨或脊柱手术后并发症很普遍,而体弱可能是导致患者并发症的一个关键因素。因此,我们评估了体弱对 30 天死亡率的影响。我们比较了风险分析指数(RAI)、改良虚弱指数-5(mFI-5)和患者年龄增加对预测 30 天死亡率的区分度。我们采用接收器操作特征曲线(ROC)研究了 RAI、mFI-5 和患者年龄增加对 30 天死亡率的分辨阈值。结果研究共纳入 19,096 名患者,在 30 天死亡率的 ROC 分析中,RAI 的判别有效性阈值 C 统计量为 0.655(95% CI:0.644-0.666),优于 mFI-5 的 C 统计量 0.570(95% CI 0.559-0.581)和患者年龄增加的 C 统计量 0.607(95% CI 0.595-0.619)。如果根据手术类型(脊柱、颅骨或其他)将患者群体分为若干子集,脊柱手术对 RAI 的判别有效性阈值最高(C 统计量为 0.717)。结论当神经外科手术后出现重大并发症时,体弱患者在 30 天内死亡的可能性高于非体弱患者。与 mFI-5 和患者年龄的增加相比,RAI 显示出更高的判别有效性阈值,使其成为一种更具临床相关性的工具,用于识别虚弱风险等级并对患者进行分层。这些研究结果突显了优化虚弱患者以减轻长期残疾的重要性。
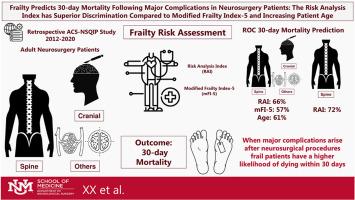
Frailty Predicts 30-day mortality following major complications in neurosurgery patients: The risk analysis index has superior discrimination compared to modified frailty index-5 and increasing patient age
Background
Postoperative complications after cranial or spine surgery are prevalent, and frailty can be a key contributing patient factor. Therefore, we evaluated frailty’s impact on 30-day mortality. We compared the discrimination for risk analysis index (RAI), modified frailty index-5 (mFI-5) and increasing patient age for predicting 30-day mortality.
Methods
Patients with major complications following neurosurgery procedures between 2012- 2020 in the ACS-NSQIP database were included. We employed receiver operating characteristic (ROC) curve and examined discrimination thresholds for RAI, mFI-5, and increasing patient age for 30-day mortality. Independent relationships were examined using multivariable analysis.
Results
There were 19,096 patients included in the study and in the ROC analysis for 30-day mortality, RAI showed superior discriminant validity threshold C-statistic 0.655 (95% CI: 0.644-0.666), compared to mFI-5 C-statistic 0.570 (95% CI 0.559-0.581), and increasing patient age C-statistic 0.607 (95% CI 0.595-0.619). When the patient population was divided into subsets based on the procedures type (spinal, cranial or other), spine procedures had the highest discriminant validity threshold for RAI (Cstatistic 0.717). Furthermore, there was a frailty risk tier dose response relationship with 30-day mortalityy (p<0.001).
Conclusion
When a major complication arises after neurosurgical procedures, frail patients have a higher likelihood of dying within 30 days than their non-frail counterparts. The RAI demonstrated a higher discriminant validity threshold than mFI-5 and increasing patient age, making it a more clinically relevant tool for identifying and stratifying patients by frailty risk tiers. These findings highlight the importance of initiatives geared toward optimizing frail patients, to mitigate long-term disability.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


