Mauro Castro-Sayat, Nicolás Colaianni-Alfonso, Luigi Vetrugno, Gustavo Olaizola, Cristian Benay, Federico Herrera, Yasmine Saá, Guillermo Montiel, Santiago Haedo, Ignacio Previgliano, Ada Toledo, Catalina Siroti
{"title":"一项前瞻性队列研究:肺部超声波评分预测接受无创呼吸支持治疗的 COVID-19 继发性急性呼吸衰竭患者的预后。","authors":"Mauro Castro-Sayat, Nicolás Colaianni-Alfonso, Luigi Vetrugno, Gustavo Olaizola, Cristian Benay, Federico Herrera, Yasmine Saá, Guillermo Montiel, Santiago Haedo, Ignacio Previgliano, Ada Toledo, Catalina Siroti","doi":"10.1186/s13089-024-00365-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lung ultrasound has demonstrated its usefulness in several respiratory diseases management. One derived score, the Lung Ultrasound (LUS) score, is considered a good outcome predictor in patients with Acute Respiratory Failure (ARF). Nevertheless, it has not been tested in patients undergoing non-invasive respiratory support (NIRS). Taking this into account, the aim of this study is to evaluate LUS score as a predictor of 90-day mortality, ETI (Endotracheal intubation) and HFNC (High Flow Nasal Cannula) failure in patients with ARF due to COVID-19 admitted to a Respiratory Intermediate Care Unit (RICU) for NIRS management.</p><p><strong>Results: </strong>One hundred one patients were admitted to the RICU during the study period. Among these 76% were males and the median age was 55 (45-64) years. Initial ARF management started with HFNC, the next step was the use of Continuous Positive Airway Pressure (CPAP) devices and the last intervention was ETI and Intensive Care Unit (ICU) admission. Of the total study population, CPAP was required in 40%, ETI in 26%, while 15% died. By means of a ROC analysis, a LUS ≥ 25 points was identified as the cut-off point for mortality(AUC 0.81, OR 1.40, 95% CI 1.14 to 1.71; p < 0.001), ETI (AUC 0.83, OR 1.43, 95% CI 1.20 to 1.70; p < 0.001) and HFNC failure (AUC 0.75, OR 1.25, 95% CI 1.12 to 1.41; p < 0.001). Kaplan-Meier survival curves also identified LUS ≥ 25 as a predictor of 90-days mortality (HR 4.16, 95% CI 1.27-13.6) and 30 days ETI as well.</p><p><strong>Conclusion: </strong>In our study, a ≥ 25 point cut-off of the Lung Ultrasound Score was identified as a good outcome prediction factor for 90-days mortality, ETI and HFNC failure in a COVID-19 ARF patients cohort treated in a RICU. Considering that LUS score is easy to calculate, a multicenter study to confirm our findings should be performed.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":"16 1","pages":"20"},"PeriodicalIF":2.9000,"publicationDate":"2024-03-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10923765/pdf/","citationCount":"0","resultStr":"{\"title\":\"Lung ultrasound score predicts outcomes in patients with acute respiratory failure secondary to COVID-19 treated with non-invasive respiratory support: a prospective cohort study.\",\"authors\":\"Mauro Castro-Sayat, Nicolás Colaianni-Alfonso, Luigi Vetrugno, Gustavo Olaizola, Cristian Benay, Federico Herrera, Yasmine Saá, Guillermo Montiel, Santiago Haedo, Ignacio Previgliano, Ada Toledo, Catalina Siroti\",\"doi\":\"10.1186/s13089-024-00365-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Lung ultrasound has demonstrated its usefulness in several respiratory diseases management. One derived score, the Lung Ultrasound (LUS) score, is considered a good outcome predictor in patients with Acute Respiratory Failure (ARF). Nevertheless, it has not been tested in patients undergoing non-invasive respiratory support (NIRS). Taking this into account, the aim of this study is to evaluate LUS score as a predictor of 90-day mortality, ETI (Endotracheal intubation) and HFNC (High Flow Nasal Cannula) failure in patients with ARF due to COVID-19 admitted to a Respiratory Intermediate Care Unit (RICU) for NIRS management.</p><p><strong>Results: </strong>One hundred one patients were admitted to the RICU during the study period. Among these 76% were males and the median age was 55 (45-64) years. Initial ARF management started with HFNC, the next step was the use of Continuous Positive Airway Pressure (CPAP) devices and the last intervention was ETI and Intensive Care Unit (ICU) admission. Of the total study population, CPAP was required in 40%, ETI in 26%, while 15% died. By means of a ROC analysis, a LUS ≥ 25 points was identified as the cut-off point for mortality(AUC 0.81, OR 1.40, 95% CI 1.14 to 1.71; p < 0.001), ETI (AUC 0.83, OR 1.43, 95% CI 1.20 to 1.70; p < 0.001) and HFNC failure (AUC 0.75, OR 1.25, 95% CI 1.12 to 1.41; p < 0.001). Kaplan-Meier survival curves also identified LUS ≥ 25 as a predictor of 90-days mortality (HR 4.16, 95% CI 1.27-13.6) and 30 days ETI as well.</p><p><strong>Conclusion: </strong>In our study, a ≥ 25 point cut-off of the Lung Ultrasound Score was identified as a good outcome prediction factor for 90-days mortality, ETI and HFNC failure in a COVID-19 ARF patients cohort treated in a RICU. Considering that LUS score is easy to calculate, a multicenter study to confirm our findings should be performed.</p>\",\"PeriodicalId\":36911,\"journal\":{\"name\":\"Ultrasound Journal\",\"volume\":\"16 1\",\"pages\":\"20\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-03-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10923765/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ultrasound Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13089-024-00365-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-024-00365-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Lung ultrasound score predicts outcomes in patients with acute respiratory failure secondary to COVID-19 treated with non-invasive respiratory support: a prospective cohort study.
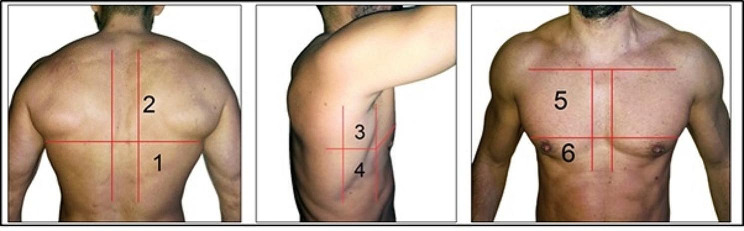
Background: Lung ultrasound has demonstrated its usefulness in several respiratory diseases management. One derived score, the Lung Ultrasound (LUS) score, is considered a good outcome predictor in patients with Acute Respiratory Failure (ARF). Nevertheless, it has not been tested in patients undergoing non-invasive respiratory support (NIRS). Taking this into account, the aim of this study is to evaluate LUS score as a predictor of 90-day mortality, ETI (Endotracheal intubation) and HFNC (High Flow Nasal Cannula) failure in patients with ARF due to COVID-19 admitted to a Respiratory Intermediate Care Unit (RICU) for NIRS management.
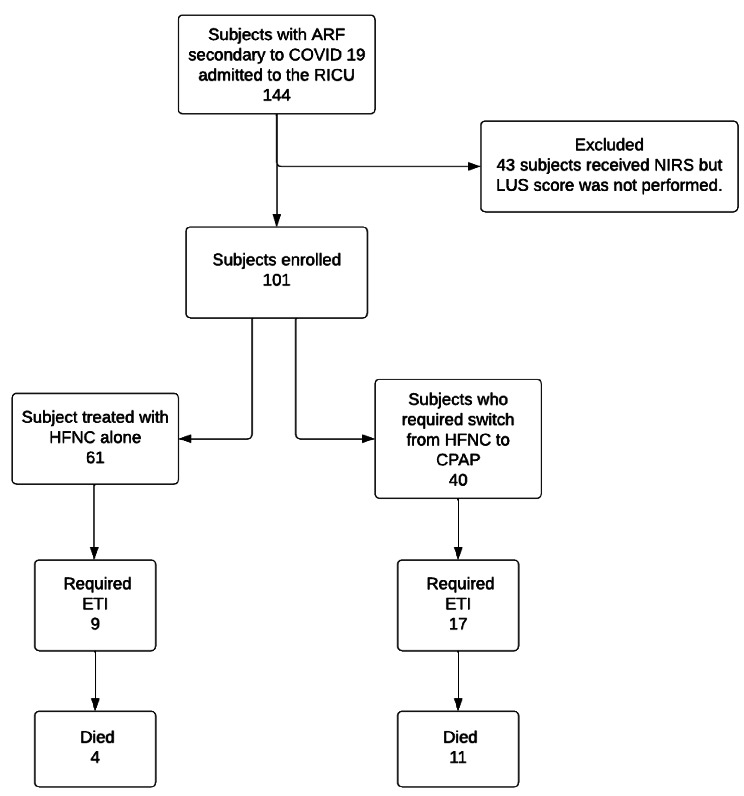
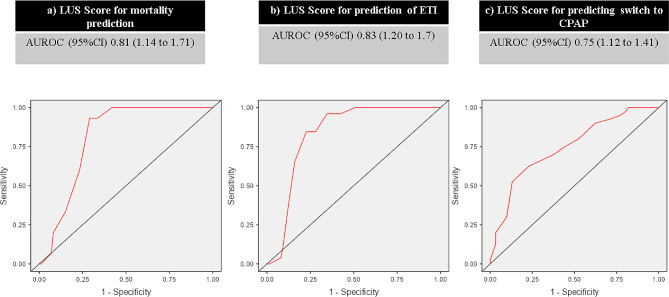
Results: One hundred one patients were admitted to the RICU during the study period. Among these 76% were males and the median age was 55 (45-64) years. Initial ARF management started with HFNC, the next step was the use of Continuous Positive Airway Pressure (CPAP) devices and the last intervention was ETI and Intensive Care Unit (ICU) admission. Of the total study population, CPAP was required in 40%, ETI in 26%, while 15% died. By means of a ROC analysis, a LUS ≥ 25 points was identified as the cut-off point for mortality(AUC 0.81, OR 1.40, 95% CI 1.14 to 1.71; p < 0.001), ETI (AUC 0.83, OR 1.43, 95% CI 1.20 to 1.70; p < 0.001) and HFNC failure (AUC 0.75, OR 1.25, 95% CI 1.12 to 1.41; p < 0.001). Kaplan-Meier survival curves also identified LUS ≥ 25 as a predictor of 90-days mortality (HR 4.16, 95% CI 1.27-13.6) and 30 days ETI as well.
Conclusion: In our study, a ≥ 25 point cut-off of the Lung Ultrasound Score was identified as a good outcome prediction factor for 90-days mortality, ETI and HFNC failure in a COVID-19 ARF patients cohort treated in a RICU. Considering that LUS score is easy to calculate, a multicenter study to confirm our findings should be performed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


