Isha Kaul, Helen Burton-Murray, Salma Musaad, Yiming Mirabile, Danita Czyzewski, Miranda A L van Tilburg, Andrew C Sher, Bruno P Chumpitazi, Robert J Shulman
{"title":"在患有胃瘫和功能性消化不良的儿童中,避免性/限制性食物摄入障碍的发病率很高。","authors":"Isha Kaul, Helen Burton-Murray, Salma Musaad, Yiming Mirabile, Danita Czyzewski, Miranda A L van Tilburg, Andrew C Sher, Bruno P Chumpitazi, Robert J Shulman","doi":"10.1111/nmo.14777","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Avoidant/restrictive food intake disorder (ARFID) prevalence in children with gastroparesis (Gp) and/or functional dyspepsia (FD) is unknown. We aimed to identify ARFID prevalence and trajectory over 2 months in children with Gp, FD, and healthy children (HC) using two screening questionnaires. We also explored the frequency of a positive ARFID screen between those with/without delayed gastric emptying or abnormal fundic accommodation.</p><p><strong>Methods: </strong>In this prospective longitudinal study conducted at an urban tertiary care hospital, patients ages 10-17 years with Gp or FD and age- and gender-matched HC completed two validated ARFID screening tools at baseline and 2-month follow-up: the Nine Item ARFID Screen (NIAS) and the Pica, ARFID, and Rumination Disorder Interview-ARFID Questionnaire (PARDI-AR-Q). Gastric retention and fundic accommodation (for Gp and FD) were determined from gastric emptying scintigraphy.</p><p><strong>Key results: </strong>At baseline, the proportion of children screening positive for ARFID on the NIAS versus PARDI-AR-Q was Gp: 48.5% versus 63.6%, FD: 66.7% versus 65.2%, HC: 15.3% versus 9.7%, respectively; p < 0.0001 across groups. Of children who screened positive at baseline and participated in the follow-up, 71.9% and 53.3% were positive 2 months later (NIAS versus PARDI-AR-Q, respectively). A positive ARFID screen in Gp or FD was not related to the presence/absence of delayed gastric retention or abnormal fundic accommodation.</p><p><strong>Conclusions & inferences: </strong>ARFID detected from screening questionnaires is highly prevalent among children with Gp and FD and persists for at least 2 months in a substantial proportion of children. Children with these disorders should be screened for ARFID.</p>","PeriodicalId":19123,"journal":{"name":"Neurogastroenterology and Motility","volume":" ","pages":"e14777"},"PeriodicalIF":3.5000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11149999/pdf/","citationCount":"0","resultStr":"{\"title\":\"Avoidant/restrictive food intake disorder prevalence is high in children with gastroparesis and functional dyspepsia.\",\"authors\":\"Isha Kaul, Helen Burton-Murray, Salma Musaad, Yiming Mirabile, Danita Czyzewski, Miranda A L van Tilburg, Andrew C Sher, Bruno P Chumpitazi, Robert J Shulman\",\"doi\":\"10.1111/nmo.14777\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Avoidant/restrictive food intake disorder (ARFID) prevalence in children with gastroparesis (Gp) and/or functional dyspepsia (FD) is unknown. We aimed to identify ARFID prevalence and trajectory over 2 months in children with Gp, FD, and healthy children (HC) using two screening questionnaires. We also explored the frequency of a positive ARFID screen between those with/without delayed gastric emptying or abnormal fundic accommodation.</p><p><strong>Methods: </strong>In this prospective longitudinal study conducted at an urban tertiary care hospital, patients ages 10-17 years with Gp or FD and age- and gender-matched HC completed two validated ARFID screening tools at baseline and 2-month follow-up: the Nine Item ARFID Screen (NIAS) and the Pica, ARFID, and Rumination Disorder Interview-ARFID Questionnaire (PARDI-AR-Q). Gastric retention and fundic accommodation (for Gp and FD) were determined from gastric emptying scintigraphy.</p><p><strong>Key results: </strong>At baseline, the proportion of children screening positive for ARFID on the NIAS versus PARDI-AR-Q was Gp: 48.5% versus 63.6%, FD: 66.7% versus 65.2%, HC: 15.3% versus 9.7%, respectively; p < 0.0001 across groups. Of children who screened positive at baseline and participated in the follow-up, 71.9% and 53.3% were positive 2 months later (NIAS versus PARDI-AR-Q, respectively). A positive ARFID screen in Gp or FD was not related to the presence/absence of delayed gastric retention or abnormal fundic accommodation.</p><p><strong>Conclusions & inferences: </strong>ARFID detected from screening questionnaires is highly prevalent among children with Gp and FD and persists for at least 2 months in a substantial proportion of children. Children with these disorders should be screened for ARFID.</p>\",\"PeriodicalId\":19123,\"journal\":{\"name\":\"Neurogastroenterology and Motility\",\"volume\":\" \",\"pages\":\"e14777\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11149999/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurogastroenterology and Motility\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/nmo.14777\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurogastroenterology and Motility","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/nmo.14777","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/7 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Avoidant/restrictive food intake disorder prevalence is high in children with gastroparesis and functional dyspepsia.
Background: Avoidant/restrictive food intake disorder (ARFID) prevalence in children with gastroparesis (Gp) and/or functional dyspepsia (FD) is unknown. We aimed to identify ARFID prevalence and trajectory over 2 months in children with Gp, FD, and healthy children (HC) using two screening questionnaires. We also explored the frequency of a positive ARFID screen between those with/without delayed gastric emptying or abnormal fundic accommodation.
Methods: In this prospective longitudinal study conducted at an urban tertiary care hospital, patients ages 10-17 years with Gp or FD and age- and gender-matched HC completed two validated ARFID screening tools at baseline and 2-month follow-up: the Nine Item ARFID Screen (NIAS) and the Pica, ARFID, and Rumination Disorder Interview-ARFID Questionnaire (PARDI-AR-Q). Gastric retention and fundic accommodation (for Gp and FD) were determined from gastric emptying scintigraphy.
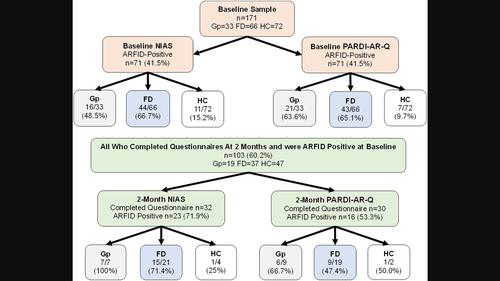
Key results: At baseline, the proportion of children screening positive for ARFID on the NIAS versus PARDI-AR-Q was Gp: 48.5% versus 63.6%, FD: 66.7% versus 65.2%, HC: 15.3% versus 9.7%, respectively; p < 0.0001 across groups. Of children who screened positive at baseline and participated in the follow-up, 71.9% and 53.3% were positive 2 months later (NIAS versus PARDI-AR-Q, respectively). A positive ARFID screen in Gp or FD was not related to the presence/absence of delayed gastric retention or abnormal fundic accommodation.
Conclusions & inferences: ARFID detected from screening questionnaires is highly prevalent among children with Gp and FD and persists for at least 2 months in a substantial proportion of children. Children with these disorders should be screened for ARFID.
期刊介绍:
Neurogastroenterology & Motility (NMO) is the official Journal of the European Society of Neurogastroenterology & Motility (ESNM) and the American Neurogastroenterology and Motility Society (ANMS). It is edited by James Galligan, Albert Bredenoord, and Stephen Vanner. The editorial and peer review process is independent of the societies affiliated to the journal and publisher: Neither the ANMS, the ESNM or the Publisher have editorial decision-making power. Whenever these are relevant to the content being considered or published, the editors, journal management committee and editorial board declare their interests and affiliations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


