Arno R Bourgonje, Martin F Bourgonje, Sara Sokooti, Sacha la Bastide-van Gemert, Tom Nilsen, Clara Hidden, Ron T Gansevoort, Douwe J Mulder, Jan-Luuk Hillebrands, Stephan J L Bakker, André P van Beek, Robin P F Dullaart, Harry van Goor, Amaal E Abdulle
{"title":"普通人群血浆钙蛋白与新发 2 型糖尿病:一项前瞻性队列研究。","authors":"Arno R Bourgonje, Martin F Bourgonje, Sara Sokooti, Sacha la Bastide-van Gemert, Tom Nilsen, Clara Hidden, Ron T Gansevoort, Douwe J Mulder, Jan-Luuk Hillebrands, Stephan J L Bakker, André P van Beek, Robin P F Dullaart, Harry van Goor, Amaal E Abdulle","doi":"10.1210/clinem/dgae130","DOIUrl":null,"url":null,"abstract":"<p><strong>Context: </strong>Systemic inflammation plays a pivotal role in the development of type 2 diabetes (T2D).</p><p><strong>Objective: </strong>We hypothesized that circulating levels of calprotectin, a myeloid cell-derived biomarker of inflammation, is associated with the development of new-onset T2D in the general population.</p><p><strong>Methods: </strong>A total of 4815 initially nondiabetic participants of the Prevention of Renal and Vascular End-stage Disease (PREVEND), a prospective population-based cohort study, were assessed for plasma levels of calprotectin at baseline. Circulating levels of calprotectin were investigated for potential associations with the risk of new-onset T2D, defined as a fasting plasma glucose level of 7.0 mmol/L or greater, a random plasma glucose level of 11.1 mmol/L or greater, a self-reported physician-based diagnosis of T2D, the use of glucose-lowering drugs, or any combinations thereof.</p><p><strong>Results: </strong>Median plasma calprotectin levels were 0.49 (0.35-0.69) mg/L. Plasma calprotectin levels were significantly associated with the risk of new-onset T2D (hazard ratio [HR] per doubling 1.42 [95% CI, 1.22-1.66]; P < .001). The association remained independent of adjustment for age and sex (HR 1.34 [95% CI, 1.14-1.57]; P < .001), but not after further adjustment for potentially confounding factors (HR 1.11 [95% CI, 0.90-1.37]; P = .326), with adjustment for hyperlipidemia and high-sensitivity C-reactive protein explaining the loss of significance. Stratified analyses showed significant effect modification by hypertension, history of cardiovascular disease (CVD), the Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) (Pinteraction ≤ .001 for each), and the use of lipid-lowering drugs (Pinteraction ≤ .05), with higher HRs in individuals without hypertension, without history of CVD, with below-median HOMA-IR, and in those not using lipid-lowering drugs.</p><p><strong>Conclusion: </strong>Elevated plasma levels of calprotectin are associated with a higher risk of developing T2D in the general population and may represent a moveable inflammatory biomarker. This association, however, does not represent a direct effect, and seems dependent on hyperlipidemia and systemic inflammation.</p>","PeriodicalId":50238,"journal":{"name":"Journal of Clinical Endocrinology & Metabolism","volume":" ","pages":"e150-e159"},"PeriodicalIF":5.1000,"publicationDate":"2024-12-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11651678/pdf/","citationCount":"0","resultStr":"{\"title\":\"Plasma Calprotectin and New-onset Type 2 Diabetes in the General Population: A Prospective Cohort Study.\",\"authors\":\"Arno R Bourgonje, Martin F Bourgonje, Sara Sokooti, Sacha la Bastide-van Gemert, Tom Nilsen, Clara Hidden, Ron T Gansevoort, Douwe J Mulder, Jan-Luuk Hillebrands, Stephan J L Bakker, André P van Beek, Robin P F Dullaart, Harry van Goor, Amaal E Abdulle\",\"doi\":\"10.1210/clinem/dgae130\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Context: </strong>Systemic inflammation plays a pivotal role in the development of type 2 diabetes (T2D).</p><p><strong>Objective: </strong>We hypothesized that circulating levels of calprotectin, a myeloid cell-derived biomarker of inflammation, is associated with the development of new-onset T2D in the general population.</p><p><strong>Methods: </strong>A total of 4815 initially nondiabetic participants of the Prevention of Renal and Vascular End-stage Disease (PREVEND), a prospective population-based cohort study, were assessed for plasma levels of calprotectin at baseline. Circulating levels of calprotectin were investigated for potential associations with the risk of new-onset T2D, defined as a fasting plasma glucose level of 7.0 mmol/L or greater, a random plasma glucose level of 11.1 mmol/L or greater, a self-reported physician-based diagnosis of T2D, the use of glucose-lowering drugs, or any combinations thereof.</p><p><strong>Results: </strong>Median plasma calprotectin levels were 0.49 (0.35-0.69) mg/L. Plasma calprotectin levels were significantly associated with the risk of new-onset T2D (hazard ratio [HR] per doubling 1.42 [95% CI, 1.22-1.66]; P < .001). The association remained independent of adjustment for age and sex (HR 1.34 [95% CI, 1.14-1.57]; P < .001), but not after further adjustment for potentially confounding factors (HR 1.11 [95% CI, 0.90-1.37]; P = .326), with adjustment for hyperlipidemia and high-sensitivity C-reactive protein explaining the loss of significance. Stratified analyses showed significant effect modification by hypertension, history of cardiovascular disease (CVD), the Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) (Pinteraction ≤ .001 for each), and the use of lipid-lowering drugs (Pinteraction ≤ .05), with higher HRs in individuals without hypertension, without history of CVD, with below-median HOMA-IR, and in those not using lipid-lowering drugs.</p><p><strong>Conclusion: </strong>Elevated plasma levels of calprotectin are associated with a higher risk of developing T2D in the general population and may represent a moveable inflammatory biomarker. This association, however, does not represent a direct effect, and seems dependent on hyperlipidemia and systemic inflammation.</p>\",\"PeriodicalId\":50238,\"journal\":{\"name\":\"Journal of Clinical Endocrinology & Metabolism\",\"volume\":\" \",\"pages\":\"e150-e159\"},\"PeriodicalIF\":5.1000,\"publicationDate\":\"2024-12-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11651678/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Endocrinology & Metabolism\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1210/clinem/dgae130\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Endocrinology & Metabolism","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1210/clinem/dgae130","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Plasma Calprotectin and New-onset Type 2 Diabetes in the General Population: A Prospective Cohort Study.
Context: Systemic inflammation plays a pivotal role in the development of type 2 diabetes (T2D).
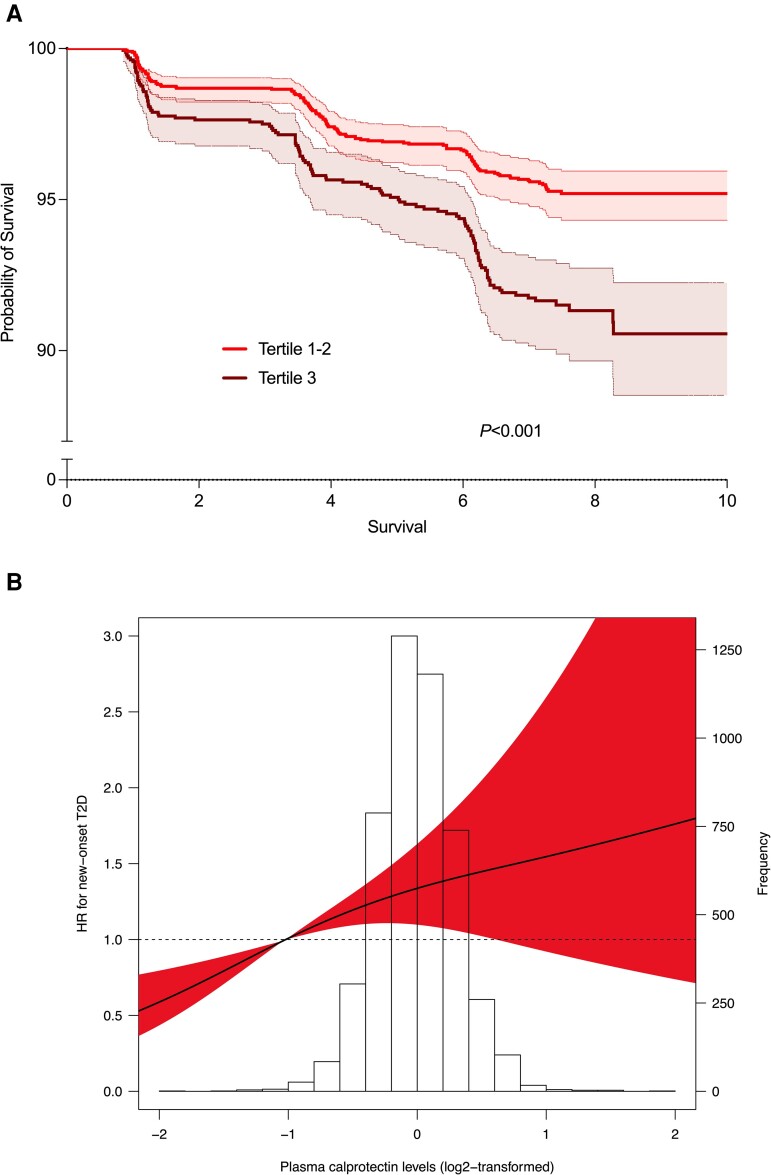
Objective: We hypothesized that circulating levels of calprotectin, a myeloid cell-derived biomarker of inflammation, is associated with the development of new-onset T2D in the general population.
Methods: A total of 4815 initially nondiabetic participants of the Prevention of Renal and Vascular End-stage Disease (PREVEND), a prospective population-based cohort study, were assessed for plasma levels of calprotectin at baseline. Circulating levels of calprotectin were investigated for potential associations with the risk of new-onset T2D, defined as a fasting plasma glucose level of 7.0 mmol/L or greater, a random plasma glucose level of 11.1 mmol/L or greater, a self-reported physician-based diagnosis of T2D, the use of glucose-lowering drugs, or any combinations thereof.
Results: Median plasma calprotectin levels were 0.49 (0.35-0.69) mg/L. Plasma calprotectin levels were significantly associated with the risk of new-onset T2D (hazard ratio [HR] per doubling 1.42 [95% CI, 1.22-1.66]; P < .001). The association remained independent of adjustment for age and sex (HR 1.34 [95% CI, 1.14-1.57]; P < .001), but not after further adjustment for potentially confounding factors (HR 1.11 [95% CI, 0.90-1.37]; P = .326), with adjustment for hyperlipidemia and high-sensitivity C-reactive protein explaining the loss of significance. Stratified analyses showed significant effect modification by hypertension, history of cardiovascular disease (CVD), the Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) (Pinteraction ≤ .001 for each), and the use of lipid-lowering drugs (Pinteraction ≤ .05), with higher HRs in individuals without hypertension, without history of CVD, with below-median HOMA-IR, and in those not using lipid-lowering drugs.
Conclusion: Elevated plasma levels of calprotectin are associated with a higher risk of developing T2D in the general population and may represent a moveable inflammatory biomarker. This association, however, does not represent a direct effect, and seems dependent on hyperlipidemia and systemic inflammation.
期刊介绍:
The Journal of Clinical Endocrinology & Metabolism is the world"s leading peer-reviewed journal for endocrine clinical research and cutting edge clinical practice reviews. Each issue provides the latest in-depth coverage of new developments enhancing our understanding, diagnosis and treatment of endocrine and metabolic disorders. Regular features of special interest to endocrine consultants include clinical trials, clinical reviews, clinical practice guidelines, case seminars, and controversies in clinical endocrinology, as well as original reports of the most important advances in patient-oriented endocrine and metabolic research. According to the latest Thomson Reuters Journal Citation Report, JCE&M articles were cited 64,185 times in 2008.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


