Kathryn Brown Holroyd, Win Min Han, Tanakorn Apornpong, Lydie Trautmann, Sivaporn Gatechompol, Akarin Hiransuthikul, Sasiwimol Ubolyam, Carlo Sacdalan, Somchai Sriplienchan, Ratchapong Kanaprach, Stephen Kerr, Anchalee Avihingsanon, Serena Spudich, Phillip Chan
{"title":"抗逆转录病毒疗法 6 年后,基于弗雷明汉风险评分的急性与慢性艾滋病队列的血管预后。","authors":"Kathryn Brown Holroyd, Win Min Han, Tanakorn Apornpong, Lydie Trautmann, Sivaporn Gatechompol, Akarin Hiransuthikul, Sasiwimol Ubolyam, Carlo Sacdalan, Somchai Sriplienchan, Ratchapong Kanaprach, Stephen Kerr, Anchalee Avihingsanon, Serena Spudich, Phillip Chan","doi":"10.1111/hiv.13621","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Immune dysregulation persists in people with HIV (PWH) on antiretroviral therapy (ART) and may lead to accelerated vascular ageing and cardiovascular disease (CVD). While delayed time to initiation of ART has been linked to worse cardiovascular outcomes, the effect of ART initiation during acute infection on these outcomes is not well understood.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Participants were enrolled from the SEARCH010/RV254 acute HIV (AHI) and HIV-NAT chronic HIV (CHI) cohorts in Thailand. Participants with 6-year follow-up and viral suppression (viral load < 50 copies/μL) at follow-up were included. Both unmatched cohorts and age and gender-matched cohorts were analysed. Demographics, HIV laboratories, and cardiovascular risk factors from enrolment and 6-year follow-up were obtained from electronic records. Framingham Risk Score (FRS), vascular age (VA), vascular age deviation (VAD), and 10-year atherosclerotic cardiovascular disease (ASCVD) risk were calculated from previously published equations. Vascular outcomes in AHI and CHI cohorts were compared, and univariable and multivariable linear regression analyses were used to investigate risk factors associated with worse vascular scores.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>In all, 373 AHI participants and 608 CHI participants were identified. AHI participants were of younger age, had a higher prevalence of syphilis and a lower prevalence of prior hepatitis B, tuberculosis, diabetes, and hypertension. Higher CD4 T-cell and lower CD8 T-cell counts were seen in the AHI cohort at enrolment and 6-year follow-up. In all participants, the AHI cohort had a lower median FRS (<i>p</i> < 0.001) and VA (<i>p</i> < 0.001), but higher VAD (<i>p</i> < 0.001). However, in matched cohorts, no differences were found in FRS-based outcomes. In all participants, higher VAD after 6 years of ART was associated with higher body mass index (<i>p</i> < 0.001) and higher CD4 count (<i>p</i> < 0.001), which persisted in multivariable analysis. When FRS components were analysed individually, CD4 count was associated only with male sex and cholesterol.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>We did not identify differences in FRS-based vascular outcomes at 6 years in matched cohorts of participants who started ART during AHI versus CHI. We identified a correlation between higher CD4 count and worse FRS-based vascular outcomes, which may be driven by underlying metabolic risk factors. Further study is needed to confirm these findings and evaluate underlying mechanisms.</p>\n </section>\n </div>","PeriodicalId":13176,"journal":{"name":"HIV Medicine","volume":"25 6","pages":"725-736"},"PeriodicalIF":2.8000,"publicationDate":"2024-02-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/hiv.13621","citationCount":"0","resultStr":"{\"title\":\"Framingham risk score based vascular outcomes in acute versus chronic HIV cohorts after 6 years of ART\",\"authors\":\"Kathryn Brown Holroyd, Win Min Han, Tanakorn Apornpong, Lydie Trautmann, Sivaporn Gatechompol, Akarin Hiransuthikul, Sasiwimol Ubolyam, Carlo Sacdalan, Somchai Sriplienchan, Ratchapong Kanaprach, Stephen Kerr, Anchalee Avihingsanon, Serena Spudich, Phillip Chan\",\"doi\":\"10.1111/hiv.13621\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>Immune dysregulation persists in people with HIV (PWH) on antiretroviral therapy (ART) and may lead to accelerated vascular ageing and cardiovascular disease (CVD). While delayed time to initiation of ART has been linked to worse cardiovascular outcomes, the effect of ART initiation during acute infection on these outcomes is not well understood.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Participants were enrolled from the SEARCH010/RV254 acute HIV (AHI) and HIV-NAT chronic HIV (CHI) cohorts in Thailand. Participants with 6-year follow-up and viral suppression (viral load < 50 copies/μL) at follow-up were included. Both unmatched cohorts and age and gender-matched cohorts were analysed. Demographics, HIV laboratories, and cardiovascular risk factors from enrolment and 6-year follow-up were obtained from electronic records. Framingham Risk Score (FRS), vascular age (VA), vascular age deviation (VAD), and 10-year atherosclerotic cardiovascular disease (ASCVD) risk were calculated from previously published equations. Vascular outcomes in AHI and CHI cohorts were compared, and univariable and multivariable linear regression analyses were used to investigate risk factors associated with worse vascular scores.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>In all, 373 AHI participants and 608 CHI participants were identified. AHI participants were of younger age, had a higher prevalence of syphilis and a lower prevalence of prior hepatitis B, tuberculosis, diabetes, and hypertension. Higher CD4 T-cell and lower CD8 T-cell counts were seen in the AHI cohort at enrolment and 6-year follow-up. In all participants, the AHI cohort had a lower median FRS (<i>p</i> < 0.001) and VA (<i>p</i> < 0.001), but higher VAD (<i>p</i> < 0.001). However, in matched cohorts, no differences were found in FRS-based outcomes. In all participants, higher VAD after 6 years of ART was associated with higher body mass index (<i>p</i> < 0.001) and higher CD4 count (<i>p</i> < 0.001), which persisted in multivariable analysis. When FRS components were analysed individually, CD4 count was associated only with male sex and cholesterol.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>We did not identify differences in FRS-based vascular outcomes at 6 years in matched cohorts of participants who started ART during AHI versus CHI. We identified a correlation between higher CD4 count and worse FRS-based vascular outcomes, which may be driven by underlying metabolic risk factors. Further study is needed to confirm these findings and evaluate underlying mechanisms.</p>\\n </section>\\n </div>\",\"PeriodicalId\":13176,\"journal\":{\"name\":\"HIV Medicine\",\"volume\":\"25 6\",\"pages\":\"725-736\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-02-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/hiv.13621\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"HIV Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/hiv.13621\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"HIV Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/hiv.13621","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
摘要
导言:接受抗逆转录病毒疗法(ART)的艾滋病病毒感染者(PWH)会持续出现免疫失调,并可能导致血管加速老化和心血管疾病(CVD)。虽然开始抗逆转录病毒疗法的时间延迟与心血管预后恶化有关,但急性感染期间开始抗逆转录病毒疗法对这些预后的影响尚不十分清楚:方法:参与者来自泰国 SEARCH010/RV254 急性 HIV (AHI) 和 HIV-NAT 慢性 HIV (CHI) 队列。随访 6 年并获得病毒抑制(病毒载量 结果)的参与者:总共确定了 373 名 AHI 参与者和 608 名 CHI 参与者。AHI 参与者年龄较轻,梅毒感染率较高,乙型肝炎、肺结核、糖尿病和高血压感染率较低。在入组和 6 年随访期间,AHI 组群的 CD4 T 细胞数量较高,CD8 T 细胞数量较低。在所有参与者中,AHI 组群的 FRS 中位数较低(p 结论:AHI 组群的 FRS 中位数较高):我们没有发现在 AHI 期间开始抗逆转录病毒疗法的匹配队列参与者与在 CHI 期间开始抗逆转录病毒疗法的匹配队列参与者在 6 年后基于 FRS 的血管预后方面存在差异。我们发现 CD4 细胞数越高,基于 FRS 的血管预后越差,这可能与潜在的代谢风险因素有关。还需要进一步的研究来证实这些发现并评估其潜在机制。
Framingham risk score based vascular outcomes in acute versus chronic HIV cohorts after 6 years of ART
Introduction
Immune dysregulation persists in people with HIV (PWH) on antiretroviral therapy (ART) and may lead to accelerated vascular ageing and cardiovascular disease (CVD). While delayed time to initiation of ART has been linked to worse cardiovascular outcomes, the effect of ART initiation during acute infection on these outcomes is not well understood.
Methods
Participants were enrolled from the SEARCH010/RV254 acute HIV (AHI) and HIV-NAT chronic HIV (CHI) cohorts in Thailand. Participants with 6-year follow-up and viral suppression (viral load < 50 copies/μL) at follow-up were included. Both unmatched cohorts and age and gender-matched cohorts were analysed. Demographics, HIV laboratories, and cardiovascular risk factors from enrolment and 6-year follow-up were obtained from electronic records. Framingham Risk Score (FRS), vascular age (VA), vascular age deviation (VAD), and 10-year atherosclerotic cardiovascular disease (ASCVD) risk were calculated from previously published equations. Vascular outcomes in AHI and CHI cohorts were compared, and univariable and multivariable linear regression analyses were used to investigate risk factors associated with worse vascular scores.
Results
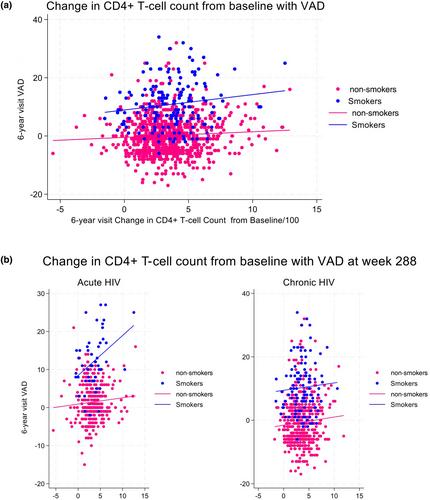
In all, 373 AHI participants and 608 CHI participants were identified. AHI participants were of younger age, had a higher prevalence of syphilis and a lower prevalence of prior hepatitis B, tuberculosis, diabetes, and hypertension. Higher CD4 T-cell and lower CD8 T-cell counts were seen in the AHI cohort at enrolment and 6-year follow-up. In all participants, the AHI cohort had a lower median FRS (p < 0.001) and VA (p < 0.001), but higher VAD (p < 0.001). However, in matched cohorts, no differences were found in FRS-based outcomes. In all participants, higher VAD after 6 years of ART was associated with higher body mass index (p < 0.001) and higher CD4 count (p < 0.001), which persisted in multivariable analysis. When FRS components were analysed individually, CD4 count was associated only with male sex and cholesterol.
Conclusions
We did not identify differences in FRS-based vascular outcomes at 6 years in matched cohorts of participants who started ART during AHI versus CHI. We identified a correlation between higher CD4 count and worse FRS-based vascular outcomes, which may be driven by underlying metabolic risk factors. Further study is needed to confirm these findings and evaluate underlying mechanisms.
期刊介绍:
HIV Medicine aims to provide an alternative outlet for publication of international research papers in the field of HIV Medicine, embracing clinical, pharmocological, epidemiological, ethical, preclinical and in vitro studies. In addition, the journal will commission reviews and other feature articles. It will focus on evidence-based medicine as the mainstay of successful management of HIV and AIDS. The journal is specifically aimed at researchers and clinicians with responsibility for treating HIV seropositive patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


